
Conclusions and Future Directions
Data presented here demonstrates that these two chronic comorbid conditions cannot be thought of as two separate and distinct entities, nor can they be treated in 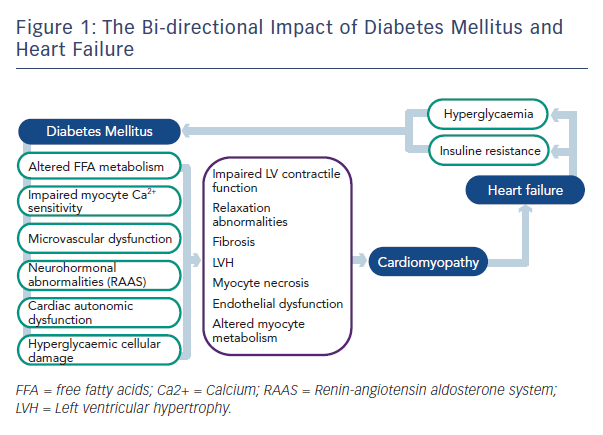 isolation. Diabetes affects myocardial glucose metabolism, cardiac fatty acid metabolism, intra-cellular calcium cycling, accelerates coronary artery disease, contributes to microvascular dysfunction, neurohormonal upregulation and increases cardiac fibrosis.20 The combination of these pathophysiological abnormalities increases the risk for developing heart failure and place added strain on an already taxed myocardium. Patients with heart failure have altered glucose metabolism and high rates of insulin resistance, increasing the risk for the development of DM. This bi-directional impact on the other disease process inexorably links these to chronic conditions together (see Figure 1). The combination of heart failure and diabetes mellitus portends worse prognosis than either comorbidity alone.
isolation. Diabetes affects myocardial glucose metabolism, cardiac fatty acid metabolism, intra-cellular calcium cycling, accelerates coronary artery disease, contributes to microvascular dysfunction, neurohormonal upregulation and increases cardiac fibrosis.20 The combination of these pathophysiological abnormalities increases the risk for developing heart failure and place added strain on an already taxed myocardium. Patients with heart failure have altered glucose metabolism and high rates of insulin resistance, increasing the risk for the development of DM. This bi-directional impact on the other disease process inexorably links these to chronic conditions together (see Figure 1). The combination of heart failure and diabetes mellitus portends worse prognosis than either comorbidity alone.
As the population of developed countries ages and the sedentary life-style, obesity rates and prevalence of hypertension increase, the prevalence of heart failure and diabetes will continue to grow. Therapies, both non-pharmacological and pharmacological, must focus on both the prevention of these devastating illnesses and on reducing their combined impact on morbidity and mortality in the population. Future research is required to address the risk and benefit of therapies directed towards each individual disease to reduce the impact on the other.