
Discussion
In the US, cardiovascular disease (CVD) mortality and incidence has decreased gradually from the 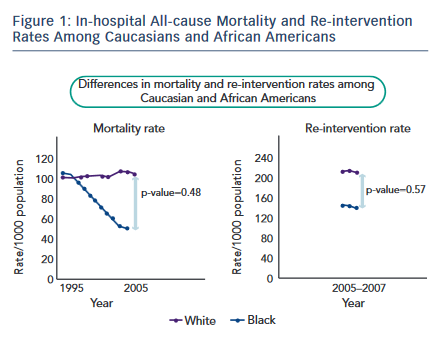 1960s onwards, though the decline has slowed down.3 In our 2007 group, the rate of patients dead was higher than in the 1997 group, which is probably due to more effective current emergency medical services and due to non-exclusion of patients presenting with cardiogenic shock and cardiopulmonary resuscitation. Risk in women lags about 5-15 years behind that of men. The average age of a person having a first coronary event is 64.5 for men and 70.3 for women.8 In our study, women were seven years older than men in the 1997 group and nine years older than men in the 2007 group (see Table 1). According to the 2011 update on heart disease and stroke statistics, the number of STEMIs are decreasing,9 but the exact incidence in young is not known. In our study, obesity and family history of CHD were major risk factors for STEMI in the young.7
1960s onwards, though the decline has slowed down.3 In our 2007 group, the rate of patients dead was higher than in the 1997 group, which is probably due to more effective current emergency medical services and due to non-exclusion of patients presenting with cardiogenic shock and cardiopulmonary resuscitation. Risk in women lags about 5-15 years behind that of men. The average age of a person having a first coronary event is 64.5 for men and 70.3 for women.8 In our study, women were seven years older than men in the 1997 group and nine years older than men in the 2007 group (see Table 1). According to the 2011 update on heart disease and stroke statistics, the number of STEMIs are decreasing,9 but the exact incidence in young is not known. In our study, obesity and family history of CHD were major risk factors for STEMI in the young.7
According to the findings of the National Conference on Cardiovascular Disease Prevention there has been a decrease in the difference in mortality rates between African Americans and the Caucasian population.3 There are other reports to suggest that the gap in CVD mortality between the various ethnic groups, poor and undereducated versus the wealthy and well-educated, has not lessened and may be widening.10 The last Cardiovascular Science and Health Care Disparities Minority Health Summit5 emphasised that racial/ethnic disparities in CVD exist and are indeed complex and multifactorial, and they occur at all levels of the medical care system. The report also mentioned that the largest difference is due to a higher mortality rate among minorities.
Although among CHD there are various reports that disparities in patient care exist,11 in our STEMI populations there was no disparity among the African American and Caucasian races in terms of mortality, length of hospital stay and cardiac re-interventions (see Table 1 and Figure 1). Our results regarding no racial disparity in the management of STEMI are in concordance with other authors.12 In the author's opinion, no racial disparity in the study is due to the systems of care in management of STEMI and to strict adherence to these treatment guidelines and protocol.
Limitations
This was a retrospective review of patients with STEMI, with a relatively small number of patients studied.