
Radial vs Femoral Access
In recent years several large registries and randomised controlled trials have demonstrated a mortality benefit for trans-radial over trans-femoral percutaneous coronary inte rvention (PCI), likely mediated by reduced bleeding complications.1–4 Building on the pioneering Japanese experience, the advent of the hybrid algorithim approach, coupled with innovative new technologies has lead to a global renewed focus and enthusiasm for chronic total occlusion (CTO) PCI with marked increase in procedural success rates.5 This approach combines the skill sets of antegrade wire escalation (AWE), antegrade dissection re-entry (ADR), retrograde wire escalation and retrograde dissection re-entry (RDR) with keen attention to minimising procedure time, contrast volume and radiation exposure (see Figure 1).
rvention (PCI), likely mediated by reduced bleeding complications.1–4 Building on the pioneering Japanese experience, the advent of the hybrid algorithim approach, coupled with innovative new technologies has lead to a global renewed focus and enthusiasm for chronic total occlusion (CTO) PCI with marked increase in procedural success rates.5 This approach combines the skill sets of antegrade wire escalation (AWE), antegrade dissection re-entry (ADR), retrograde wire escalation and retrograde dissection re-entry (RDR) with keen attention to minimising procedure time, contrast volume and radiation exposure (see Figure 1).
Arterial Access in CTO PCI
One challenge, however, in CTO PCI remains the risks of multiple and larger vascular access. Whilst for conventional PCI the direction of travel is towards miniaturisation with smaller French sizes and sheathless approaches,6 in CTO PCI, larger French systems are required to offer capability across the full spectrum of techniques (see Table 1). In addition, CTO procedures are often dependent on visualisation of the occluded vessel by contra-lateral collaterals requiring dual access sites and contra-lateral coronary injection hence immediate potential to double the risks of access complication. Furthermore the thrombotic risk of equipment in both coronary circulations requires meticulous anticoagulation management with a target activated clotting time (ACT) greater than 300s measured systematically every 20–30 minutes. This contrasts with a target of 250s for conventional single access site non-CTO PCI and might exacerbate any access related bleed.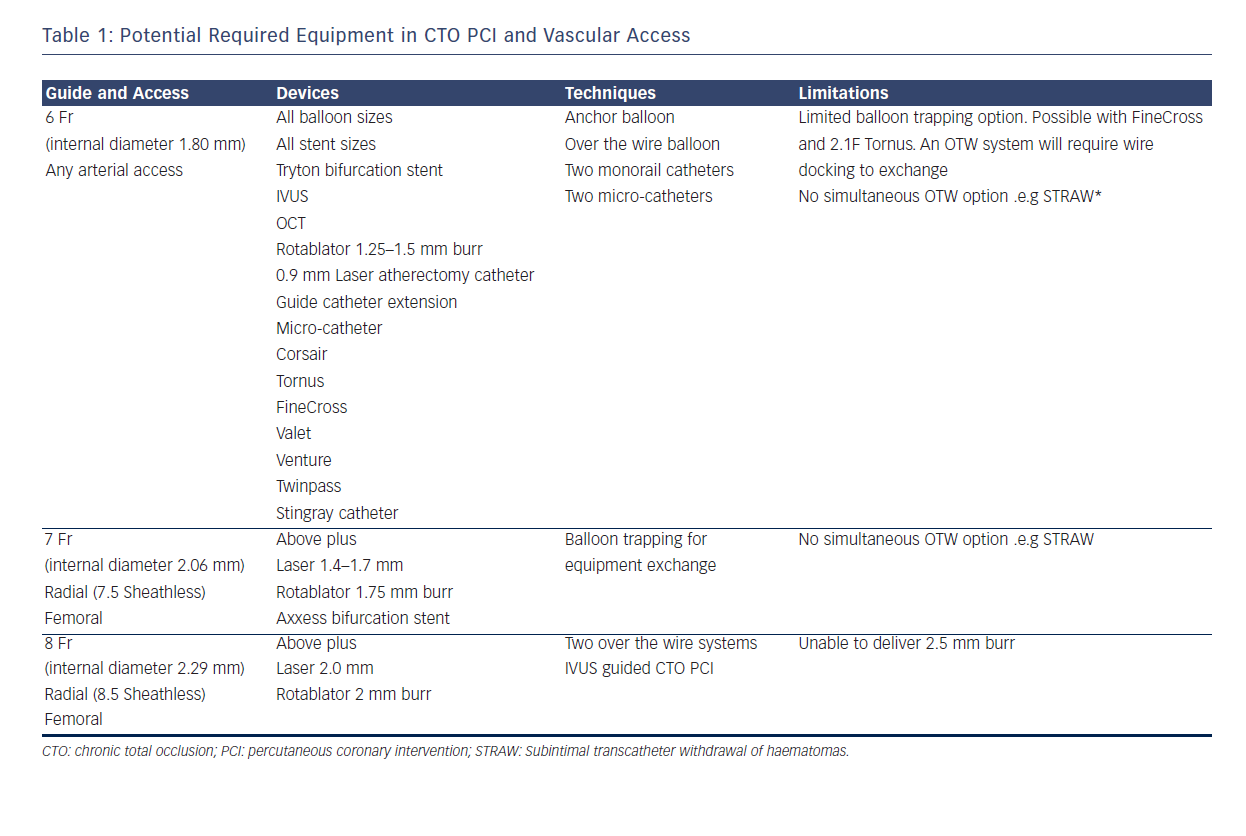
Table 1 describes the procedural techniques as accommodated by different guide catheter sizes. 8F is required to accommodate two over-the-wire (OTW) technologies and also offers greater passive guide catheter back-up to facilitate penetration of the CTO proximal cap, an essential step and when unsuccessful, a frequent mode of failure. The radial and ulnar arteries infrequently have an inner luminal diameter larger than 2.5 mm in men at the wrist making insertion of a 7F sheath (outer diameter 3.06 mm) a usual maximum in men and 6F sheath (outer diameter 2.67 mm) in women.7,8 The requirement for an 8F system has resulted in CTO PCI bucking the trend towards trans-radial PCI with high use of trans-femoral access. This has implications for training of medical and nursing staff (operative and after care) in increasingly radial dominant centres. Below we discuss the evidence for best practice with respect to femoral puncture technique and also assess the technologies and techniques available to place larger inner diameter catheters into the radial artery.