
In the PRAMI trial the evidence of benefit emerged early on.24 The curves in the Kaplan–Meier plot (see Figure 2) diverged within a few days and the maximum effect was evident within a few months, suggesting that the immediacy of preventive PCI is important and that staged preventive PCI (undertaken after a few weeks) may not be as effective. The same observations were apparent in the Complete Versus culprit-Lesion only PRimary PCI Trial (CVLPRIT) trial22 in which all but about a quarter of patients in the preventive PCI group had immediate preventive PCI, the remainder having a staged procedure within a few days. Neither of the two trials was designed to compare immediate versus staged preventive PCI. Such a trial, if judged necessary, would need to be large to demonstrate a difference in outcome on top of the 60 % reduction in cardiac death or MI from preventive PCI alone.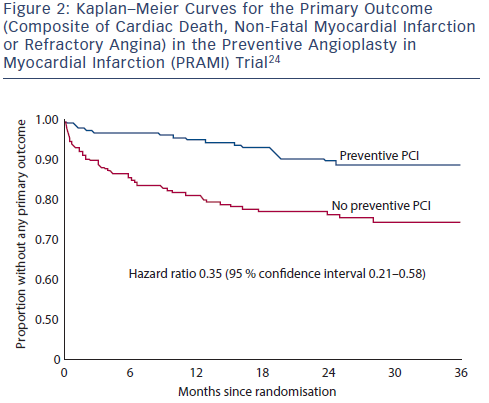
The results of PRAMI24 and CvLPRIT22 have prompted a rethink in the way we manage non-infarct artery stenoses in STEMI. The European Revascularisation Guidelines were recently changed (September 2014) and now recommend that immediate preventive PCI be considered in selected patients with STEMI,37 but do not indicate how this selection should be made. The use of a physiological measure of blood flow, such as fractional flow reserve (FFR), may be better than visual angiographic assessment in guiding preventive PCI,38 but it may also worsen outcomes if non-flow limiting stenoses are left untreated and become the sites of future infarction. Three trials of preventive PCI in patients with STEMI are in progress that are using FFR to decide which non-infarct artery stenoses to treat.39–41 No trial is designed to directly compare FFR with angiography in STEMI to determine which, if either, is better in guiding preventive PCI. Further research would be needed to resolve this uncertainty.
A limitation of the trials of preventive PCI, as in all randomised trials, is that they only provide an average effect of treatment. Some patients will benefit more from preventive PCI than others, but in the absence of knowing who they are, no special selection can be recommended. The trials excluded patients with cardiogenic shock, previous coronary artery bypass graft (CABG), significant stenosis of the left main stem or in whom the only non-infarct artery disease was a chronic total occlusion. Therefore, while the benefits of preventive PCI may apply in these selected groups, there is uncertainty. In others, for whom the non-infarct artery stenoses are judged treatable by PCI, the evidence from the trials completed so far, is clear – that immediate preventive PCI confers substantial clinical benefit. The primacy of randomised trials reveals the danger of using non-randomised studies, which can, as in this case, give the wrong answer.