
The Epidemiology of Heart Failure with Preserved Ejection Fraction
Figure 1 shows patients admitted to European hospitals with a diagnosis of HF. As we can see high EFs are just as likely as low, especially in females where they form the 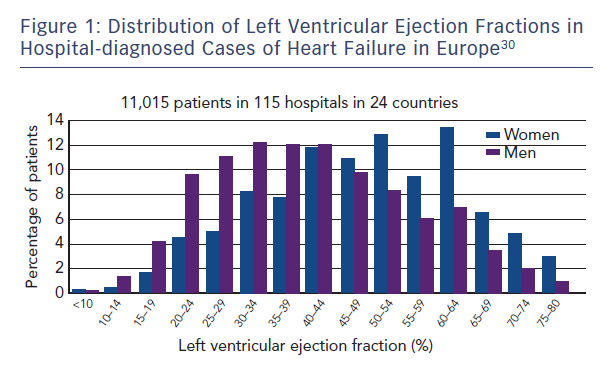 majority.
majority.
Multiple epidemiological studies have suggested a prevalence of HF in western developed countries of between 1–2 % of the adult population,2 with a steeply increasing prevalence of HF with increasing age. More than 50 % of patients who ever develop HF will do so for the first time over the age of 75 years. Age is also of major importance in predicting the type of HF a patient is likely to present with. HR-REF predominates in younger patients and is most commonly secondary to coronary artery disease. The major RCTs of HF therapy have mainly recruited younger patients, with a mean age of 61 years in all the beta-blocker trials prior to SENIORS, which specifically targeted an older population. This is a decade and half younger than the average age in the community. The older patient, by contrast, is more likely to have hypertension as the predominant aetiology factor, to be female and to have the HF-PEF pattern of LV physiology. There has not been a single mortality and morbidity RCT of HF with an average age of recruits older than 76 years. The mortality of HF-PEF is said by many reports from hospital case series and clinical trials to be lower than that of HF-REF, suggesting it is a condition of lesser importance. In fact in large epidemiological studies in a community setting, or rigidly performed on a sound epidemiological basis, the prognosis of HF-PEF is virtually indistinguishable from that of HF-REF. The most worrying feature is that over the last 15 years only for HF-REF has there been any improvement in the risk of mortality, for HF-PEF it has remained unchanged. This period coincided with one of the most significant advances in the therapy of cardiovascular disease (CVD), the revolution in our treatmen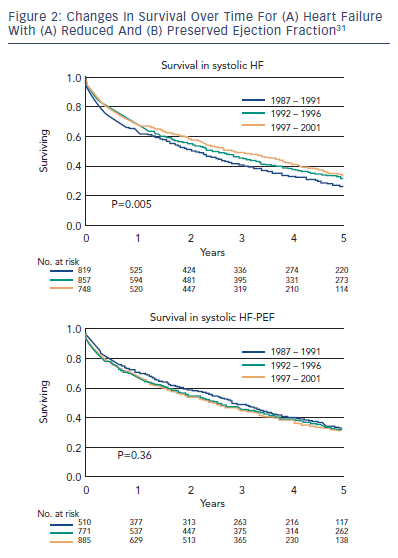 t of chronic HF (CHF). Consecutively hospitalised decompensated HF patients at Mayo Clinic Hospitals in Olmsted County, Minnesota, US, from 1987 through 2001 show that over this period the proportion with HF-PEF has gone from just below 50 % to more than 50 % and that in contrast to HF-REF there has been no increase in long-term survival.3 See also Figure 2.
t of chronic HF (CHF). Consecutively hospitalised decompensated HF patients at Mayo Clinic Hospitals in Olmsted County, Minnesota, US, from 1987 through 2001 show that over this period the proportion with HF-PEF has gone from just below 50 % to more than 50 % and that in contrast to HF-REF there has been no increase in long-term survival.3 See also Figure 2.
More recent reports similarly show outcomes as poor for HF-PEF as for HF-REF.4 The reports that have been said to show much better prognosis of HF-PE compared with HF-REF patients are more commonly series of patients specifically investigated and chosen to enter clinical trials, where other co-morbidities (common in the elderly) are often exclusion criteria. Some reports of this nature suggest that survival is significantly better for HF-PEF compared with HF-REF,5 such as analyses comparing two different clinical trials, such as CHARM Preserved versus the two other CHARM studies, and such analyses also suggest prognostic6,7 and pathophysiological factors may be distinct;8–12 however, these comparisons are biased by the fact that recruitment to trials itself is biased against patients with HF-PEF. That is because trials exclude many patients on the basis of confounding co-morbidities, by the reasoning that co-morbidities confound the trial’s evaluation of a treatment on one condition. But if co-morbidities are, by their natural history, common in a certain disease state then excluding patients with these co-morbidities you are selecting for a very biased and unrepresentative group of patients. This cannot be corrected by analysing ever-larger numbers. We can only compare the outlook and prognosis of HF-PEF and HF-REF by recruiting patients from epidemiologically valid or whole population cohorts, not by analysing selected clinical trial cohorts. The mortality rate of trial HF-PEF patients is lower than that of HF-PEF trial patients because so many of the higher risk HF-PEF patients are excluded to find a ‘purer’ form of HF-PEF. Epidemiologically sound studies find the prognosis of HF-PEF and HF-REF are virtually indistinguishable. Early trials such as the DIG13 trial of digoxin recruited HF patients of both HF-PEF and HF-REF subtypes (sometimes called the DIG-REF trial and the DIG HF-PEF trial) and the effects were similar for the types. Later trials, in the interest of increasing event rates, over-recruited HF-REF and many restricted entry to patients with a LVEF less than 45 %, 40 %, 35 % or even lower (25 % for Copernicus).14 This was done to increase mortality rates, but had the effect of leaving HF-PEF patients unstudied and hence many years later untreated.
Clinical Treatment Trials in Heart Failure with Preserved Ejection Fraction
There have been remarkably few M+M RCTs in HF-PEF. These trials are of two types. In one type, all HF is recruited into a M+M trial and subsets include HF-PEF and HF-REF type patients. The trial is powered to establish its primary efficacy analysis based on the whole trial population then we investigate important subgroups to see if the treatment effect is statistically significantly (or even trending to) different in these subgroups. Occasionally, a subgroup treatment effect may be statistically significant in its own right, but this is not the principal analysis. The best estimate of the treatment effect in a subgroup, if there is no significant effect treatment/subgroup interaction, is that of the whole trial result itself. By this measure if the trial is positive, and if the HF-PEF patients show a similar result and no statistically interaction with treatment, then this is considered evidence the treatment also works in that subgroup, provided of course there are reasonable numbers and not just a handful.
The second type is the standalone trial powered for and recruiting only HF-PEF type patients. In contrast to over 100 such trials in HF-REF there have only been four such trials: CHARM-Preserved, PEP-CHF, I-Preserve and TOPCAT that will be reviewed below.