
 Two Scaffolds Strategy
Two Scaffolds Strategy
Historically, a two-stent approach has never been demonstrated to be superior to the provisional approach. A more complex bifurcation lesion, especially with significant obstructive atherosclerosis in both the main branch and a >2.5 millimetres (mm) side branch (so-called Medina 1,1,1) may warrant a multiple device technique.
The culotte technique evolves with stenting one leg of the bifurcation, rewiring and ballooning into the other leg, followed by stenting of the uncovered branch through the first stent and completed with kissing balloon inflations. This translates into a proximal segment of the main vessel covered with two overlapping stents and in principle good coverage of the carina.23 The culotte technique fits best when there is only a limited sizing mismatch between the branches. Our group recently reported procedural feasibility of the culotte technique with BVS (see Figure 2).24 BVS can be appealing with this technique since over time the scaffolds will resorb, avoiding a permanent multilayer of metal in the coronary artery, leaving a smooth carina. This concept may virtually eliminate persistent device-malapposition or delayed healing at the side branch ostium, theoretically impacting on the incidence of thrombosis. Conversely, the implantation procedure per se could be hindered by the relatively high crossing profile of the BVS often requiring an optimal back-up guide catheter, highly supportive wires and a relatively aggressive preparation and dilatation of the bifurcation substrate and the initial scaffold.
The crush and mini-crush technique consists by design of crushing and deforming the proximal protruding segment of the side branch scaffold, followed by a second scaffold implantation. Afterwards the side branch needs to be rewired through three layers of cells to complete the technique with kissing balloon inflations. In the context of BVS the impact of crushing the polymeric polylactic acid struts is unknown; it is debatable in fact whether the crushing would be associated with intrinsic fractures that may jeopardise the overall scaffold integrity. In vitro observations are needed to fully evaluate the morphology and the integrity of the BVS after crushing.
 The V-technique implies the delivery and simultaneous implantation of two devices. One scaffold is advanced in the side branch, the other in the main branch forming a proximal carina.25 The V-technique is particularly suitable for bifurcations with medina classification 0,1,1. If correctly executed, struts will not jail the access to either of the two branches with no need for struts re-crossing. This can be an attractive aspect considering BVS with its higher profile and 150 µm strut thickness.
The V-technique implies the delivery and simultaneous implantation of two devices. One scaffold is advanced in the side branch, the other in the main branch forming a proximal carina.25 The V-technique is particularly suitable for bifurcations with medina classification 0,1,1. If correctly executed, struts will not jail the access to either of the two branches with no need for struts re-crossing. This can be an attractive aspect considering BVS with its higher profile and 150 µm strut thickness.
In a variable percentage (up to 30 %) of cases treated with a provisional approach a cross-over to a two-stent technique is required. The T-stenting and small protrusion (TAP) approach26,27 is a relatively new technique, ensuring complete coverage of the side branch ostium minimising stent overlap. Technically, the TAP technique is less challenging compared with reverse culotte and reverse crush, and is feasible in a variation of bifurcation angulations (at variance of reverse T-stenting that can only be optimally performed in bifurcations with 90° angulation). TAP technique may be challenging with BVS as re-crossing and dilatation of scaffold struts into the side branch are necessary. A potential disadvantage of the TAP technique is the presence of struts protruding into the main vessel lumen that occasionally impair laminar blood flow in the main vessel. Interestingly, in this setting, BVS may have the unique advantage of a complete coverage of the side branch ostium with an eventual complete disappearing of the protruding struts over time.
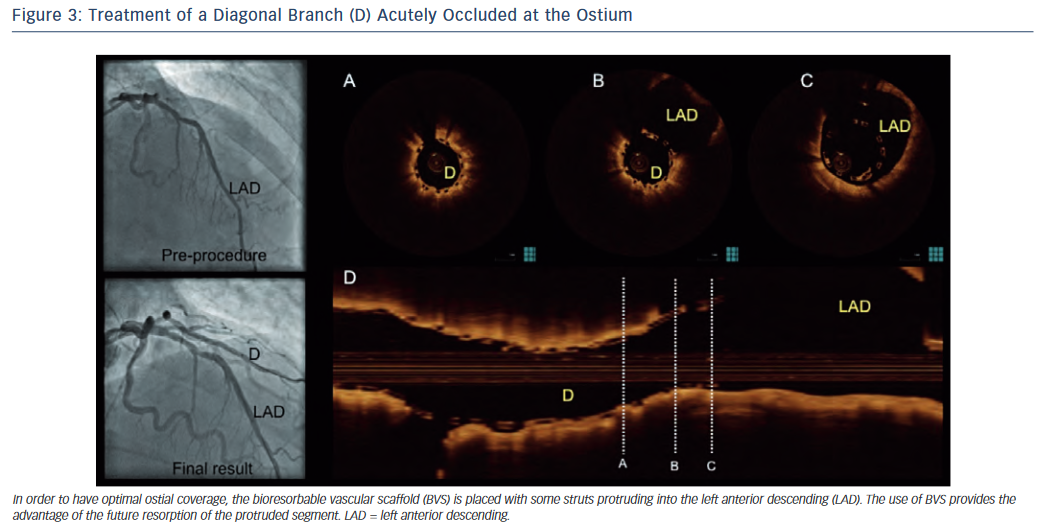
Finally, in ostial lesions (e.g. aorto-ostial, ostium left anterior descending lesions, ostium circumflex lesions and bifurcations medina 0,0,1) BVS can be an interesting product as complete ostium coverage can be achieved with only temporary strut protrusion into the aorta or main vessel (see Figure 3).