
Valve-in-Valve
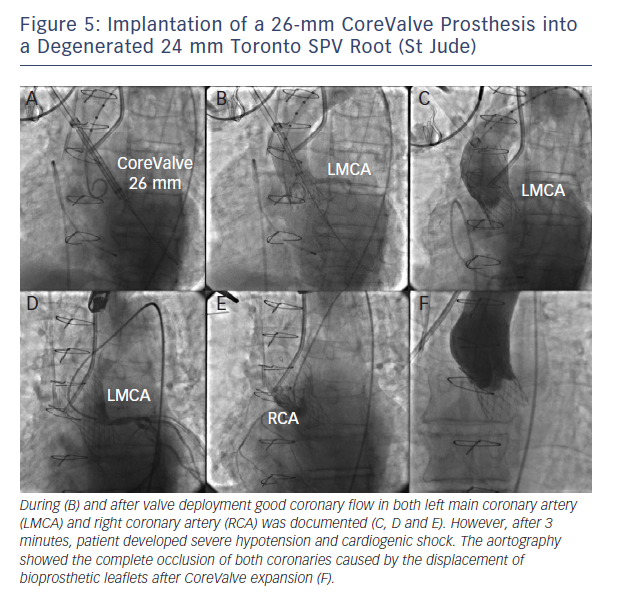
Coronary obstruction is three- to fourfold more common after TAVI in degenerated surgical bioprostheses compared with native valve TAVI.15 Recently, Dvir and colleagues reported a coronary obstruction incidence of 3.5 % of patients.15 The main predisposing factor in the setting of aortic valve-in-valve procedures is the proximity of the coronary ostia to the anticipated final position of the displaced bioprosthetic leaflets after THV implantation. Therefore, predisposing factors for coronary obstruction may include a supra-annular bioprosthetic valve, a narrow and low-lying sinotubular junction, bulky bioprosthetic leaflets, low-lying coronaries in narrow aortic root and reimplanted coronaries.15 Bearing these concepts in mind, it appears logical that stentless bioprosthetic valves or those that are internally stented (eg, Mitroflow, Sorin; Trifecta, St Jude Medical) may be at a higher risk because the leaflets of these bioprostheses may extend outward in a tubular fashion after valve implantation beyond the surgical device frame (see Figure 5).15,16 In this setting, meticulous fluoroscopic and cardiac MDCT assessment may identify most cases at risk.16