
Ventricular tachycardia (VT) is a significant cause of morbidity and mortality in patients with structural heart disease (SHD). While implantable cardioverter-defibrillators 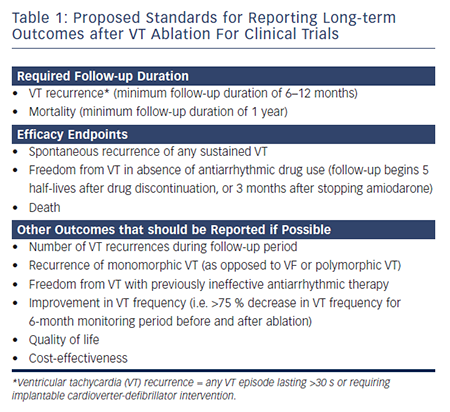 (ICDs) have been shown to be effective in preventing sudden death due to ventricular arrhythmias, they are not able to prevent recurrent VT episodes. Antiarrhythmic drugs (AADs) have some demonstrated efficacy in preventing VT episodes, although options remain limited in patients with SHD and the degree of benefit is suboptimal. Amiodarone is the most effective AAD, but is associated with significant side-effects with long-term use, and many patients are unable to tolerate the medication.
(ICDs) have been shown to be effective in preventing sudden death due to ventricular arrhythmias, they are not able to prevent recurrent VT episodes. Antiarrhythmic drugs (AADs) have some demonstrated efficacy in preventing VT episodes, although options remain limited in patients with SHD and the degree of benefit is suboptimal. Amiodarone is the most effective AAD, but is associated with significant side-effects with long-term use, and many patients are unable to tolerate the medication.
With the advances in technology over the past two decades, catheter ablation has become an increasingly utilised adjunctive treatment modality for patients with VT. Catheter ablation has been clearly shown to be effective in decreasing the number of VT episodes, including antitachycardia pacing (ATP) therapies and shocks. While catheter ablation reduces long-term VT recurrences, it has not been shown to provide mortality benefit in patients with SHD.1 In this regard, patients still tend to be referred for ablation late in their disease course. Two prior studies have shown that early referral for ablation in patients with ischaemic and non-ischaemic cardiomyopathy (ICM and NICM) is associated with improved long-term VT suppression.2,3
There have been limited data published from prospective randomised controlled trials examining the long-term outcomes of VT ablation. Most outcome studies have been single or multicentre retrospective observational experiences, and case series with limited sample sizes, so are subject to a variety of biases and confounding factors.
In this article, we will summarise the available data on long-term outcomes following VT ablation in patients with different types of SHD.
Heterogeneity of Ventricular Tachycardia Ablation Studies – Impact on Long-term Outcomes
The 2009 VT ablation guidelines have proposed standards for reporting long-term outcomes after VT ablation for clinical trials (see Table 1).4 However, the outcomes in previous smaller retrospective studies have been quite variable. The patient populations in different studies may vary significantly with regards to the number of VT episodes, haemodynamic stability of VTs, presence of back-up ICD, etc. Additionally, ablation strategies (i.e. endocardial versus endocardial/epicardial approach; mapping and ablation approaches) may differ between studies, based on investigator and institutional preferences. Substrate-based ablation approaches, which are often used in patients with haemodynamically unstable VT, may differ greatly between VT ablation centres (i.e. late potential ablation, local abnormal ventricular activity ablation, scar homogenisation, scar dechannelling, linear ablation strategies and core isolation).5–12 When VT recurs after an initial ablation procedure, repeat ablation may be necessary to achieve long-term suppression.13 While some studies report long-term outcomes following the index ablation procedure, others have referred to long-term outcomes following the last ablation procedure in patients requiring multiple procedures. Therefore, it is of utmost importantance that providers carefully review the methods of each study, particularly inclusion and exclusion criteria, prior to extrapolating results to individual patients in clinical practice.