
Unfortunately, the most enthusiastic proponents of RDN do not seem to have fully accepted the lessons of Symplicity HTN-3. In the aftermath of Symplicity HTN-3, a campaign has been set up to criticise the study because of including inexperienced investigators, who did not appropriately document the delivery of ablation energy in the renal arteries, and enrolling too many African American patients who improved their drug adherence in the course of the trial.31,44 Symplicity HTN-3 may have had its weaknesses, however, no subgroup analysis was statistically significant4 and all the hypotheses explaining the failure of Symplicity HTN-3 by showing a difference in blood pressure were post hoc and speculations. Besides, also this study was overseen by procedure experts (proctors) from the sponsoring company, namely Medtronic. Furthermore, the Symplicity HTN-3 results are diluted by non-scientific comparisons with the Medtronic® registry45 which is hampered by all the weaknesses touched upon in this commentary, and even more as it is a pure industry-ran activity. Finally, while RDN will not become available in the US, and ongoing research in Asia was stopped, Medtronic and other companies continued making their catheters available for clinical use in Europe and did not restrain from heavily promoting the technique, for example at the Euro PCR conference in Paris in May 2014 (www.medscape.com/author/shelley-wood).
One-year results of Symplicity HTN-34 were presented at the European Society of Cardiology (ESC) meeting in Barcelona in end of August 2014. Following the six-month evaluation all subjects and clinicians were unblinded and antihypertensive medications changes were allowed. Of the 171 original sham control group subjects, 101 who still fulfilled all of the baseline inclusion and exclusion criteria, and agreed to receive the procedure, crossed over to RDN. The remaining 70 sham control subjects did not cross over and were not treated with RDN. At one year post-procedure, both office and 24 hour mean ambulatory systolic blood pressure continued to demonstrate a decrease in the original RDN group. Similarly, the crossover group showed blood pressure reductions six months following RDN (Δ systolic blood pressure: 17.7 mm Hg, P<0.001). The non-crossover group also had large reductions in office pressure one year post randomisation (Δ systolic blood pressure: 21.4 mm Hg, P<0.001) (http://congress365. escardio.org/). In the summary session of the ESC meeting the keynote speaker (Bryan Williams, London, U.K.) on September 3 pointed out the uncertain future of RDN based on the recent randomised studies performed in Oslo38 and in the US.4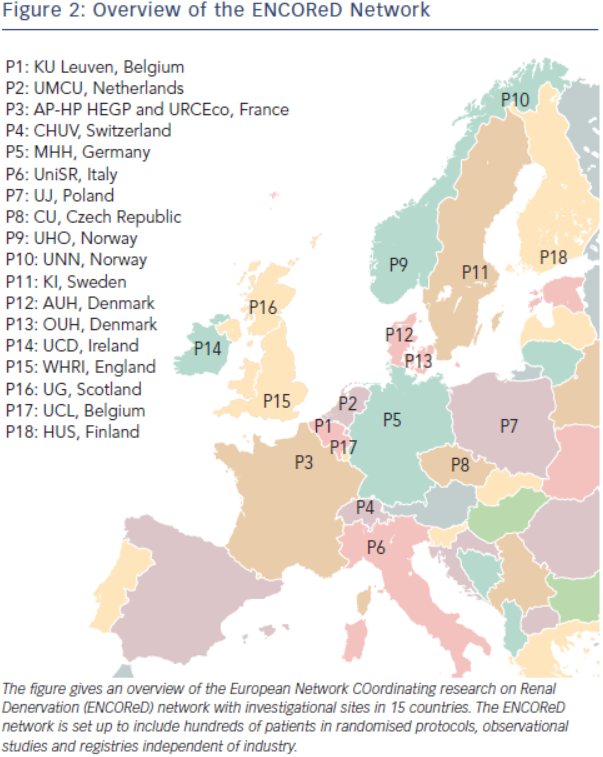
The key message of Symplicity HTN-34 is simple and we should be wise enough to accept it: the true overall benefit of RDN on systolic blood pressure is modest, <3 mmHg, without evidence of a favourable impact on morbidity-mortality so far. The results of three other recent rigorously designed randomised controlled trials, Oslo RDN38 (see Table 1), DENER-HTN46, and PRAGUE-1547 including a smaller number of well-trained operators are in line with those of Symplicity HTN-34, and confirm that the failure of RDN to achieve superiority over medical treatment in the latter cannot be merely explained by inclusion of a high proportion of African Americans or insufficient degree of renal nerve ablation. Along the same lines, a fourth randomised shamcontrolled study performed in mild resistant hypertension (daytime systolic blood pressure between 135 and 149 mmHg and/or diastolic blood pressure between 90 and 94 mmHg on ≥ 3 drugs classes including a diuretic), Symplicity Flex48, failed to show an advantage of RDN compared to drug treatment alone.
Does the failure of Symplicity HTN-3 mean the end of RDN? Not necessarily. Indeed, as already mentioned, RDN is based on a solid rationale substantiated by over fifty years of meticulous research of the sympathetic nervous system and its involvement in the pathophysiology of hypertension.6–12 Furthermore, it has been shown in cohorts recruited from the third (The effect of progressive sympathectomy on blood pressure, Walter Bradford Cannon 1931, http://www.ncbi.nlm.nih.gov/ pubmed/2204236) until the fifth decade of the last century49,50 that abdominal sympathectomy associated to splanchnicectomy is effective in the treatment of severe hypertension. Finally, many centres report major responses to RDN in a minority of patients.33,35,38 Accordingly, research should go on to find out the minority of patients who are true responders to RDN, and identify predictors of effective RDN. The ENCOReD network (see Figure 2) is set up to include hundreds of patients in randomised protocols, observational studies and registries independent of industry. Some early results35,51 from this joint effort have already been published and suggest that it may be worthwhile searching for potential predictors of response to RDN.