
Symptomatic severe aortic stenosis or insufficiency have no effective medical treatments and carry a dismal prognosis if left untreated. Since the first aortic valve replacement in 1960, hundreds of thousands of lives have been saved and improved by this procedure. Until recently, surgical aortic valve replacement (sAVR) was the only effective therapy for severe aortic valve stenosis. The recent introduction of transcatheter aortic valve replacement (TAVR) has offered an alternative in specific high-risk patients with symptomatic severe aortic stenosis. The rapid adoption and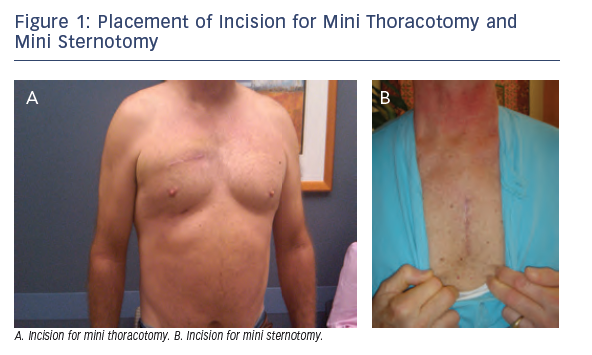 dissemination of TAVR have led some to speculate on the demise of sAVR. Although TAVR has and will continue to cater to a portion of patients with aortic valve disease, in the meantime, the field of sAVR has not stood stagnant but rather continues to advance and improve in tandem with TAVR. In addition to surgical valve replacement techniques, repair principles have been adopted from the mitral valve to the aortic valve with growing success leading to the standardization of regurgitant aortic valve repair approaches. This article will examine the current surgical approaches for aortic valve replacement with insights into the challenges faced and how these approaches will remain competitive with catheterbased technologies. We will focus on minimally invasive approaches to sAVR, new valve technologies, and aortic valve repair techniques.
dissemination of TAVR have led some to speculate on the demise of sAVR. Although TAVR has and will continue to cater to a portion of patients with aortic valve disease, in the meantime, the field of sAVR has not stood stagnant but rather continues to advance and improve in tandem with TAVR. In addition to surgical valve replacement techniques, repair principles have been adopted from the mitral valve to the aortic valve with growing success leading to the standardization of regurgitant aortic valve repair approaches. This article will examine the current surgical approaches for aortic valve replacement with insights into the challenges faced and how these approaches will remain competitive with catheterbased technologies. We will focus on minimally invasive approaches to sAVR, new valve technologies, and aortic valve repair techniques.
Minimally Invasive Surgical Aortic Valve Replacement
sAVR requires the use of the heart lung machine to stop the heart and to allow access to the aortic valve within the heart. The traditional approach to exposing the heart for bypass and to gain access to the aortic valve has been via median sternotomy. Median sternotomy allows excellent access to all cardiac structures but requires complete division of the sternum and sternal spreading. This disrupts the integrity of the chest wall in the early recovery phase. Surgeons therefore decided to look for less invasive ways of performing sAVR to see if this would lead to easy recovery and possibly improved results for patients. The parasternal approach to sAVR was first reported by Cosgrove in 1996, but has been largely abandoned due to chest wall hernias.1 The right mini thoracotomy approach was introduced by Benetti in 19972 and the mini sternotomy approach by Gundry in 1998.3 At the Houston Methodist Hospital, we began our minimally invasive valve program in 1999 when we performed anatomic studies on cadavers. In these studies, we examined the relationship of the cardiac valve structures to the chest wall to help plan potential surgical approaches.4 From these early studies in our program, we have employed two minimally invasive approaches to sAVR: mini sternotomy and mini thoracotomy (see Figure 1).