
Practical Strategic Synthesis for the Use of Different Invasive Diagnostic Exploration Techniques 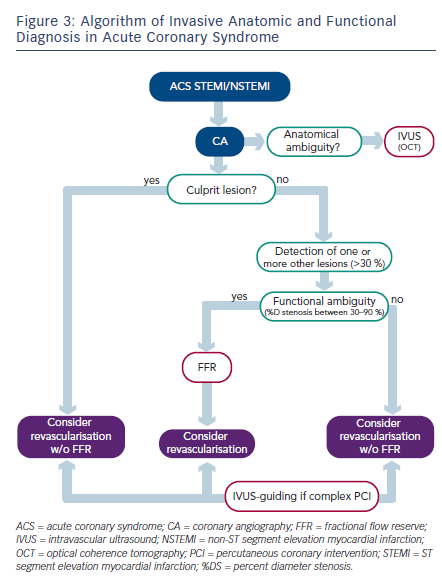
Coronary angiography is the foundation of any invasive exploration, rapidly and reliably detecting whether any coronary lesion is present or not.
However, anatomic descriptive (or qualitative) analysis of the angiogram may be difficult or ambiguous – realtime invasive cross-sectional imaging with high spatial resolution, depth exploration going beyond the adventitia and a single complete acquisition of the entire epicardial arterial axis is then indispensable. IVUS meets these requirements, usefully complementing angiography.42
Functional analysis of coronary stenosis needs to be definitively freed from lesion anatomy, and requires a specifically dedicated technique for each patient, artery and lesion. Pressure guide determination of FFR fully meets these requirements, and should be implemented in all intermediate (30–90 %DS) lesions.3
Twenty years ago, many interventional cardiologists, already aware of the limitations of CA, were imagining the advent of new complementary anatomic and functional techniques.8 Now in 2013, such techniques are actually available. Two major complementary techniques have been developed and received wide scientific validation, with precise recommendations – IVUS and FFR.
Algorithms for the Implementation of Complementary Invasive Diagnostic Techniques
In everyday interventional cardiology, several algorithms may guide the implementation of these two complementary techniques: functional (using FFR) and anatomical (using IVUS or OCT).
Most patients undergoing CA have not had prior non-invasive functional testing.43,44 The functional ambiguity of any coronary lesions found on CA will then be unattenuated (see Figure 1).
Even if non-invasive functional testing is performed ahead of CA, functional ambiguities may still appear in cases of multiple lesions on one or more coronary arteries (single or multivessel disease). Another problem recently emerged, the value of non-invasive testing for location purposes. While effort tests do not help with location, myocardial scintigraphy and stress echo are claimed to do so. 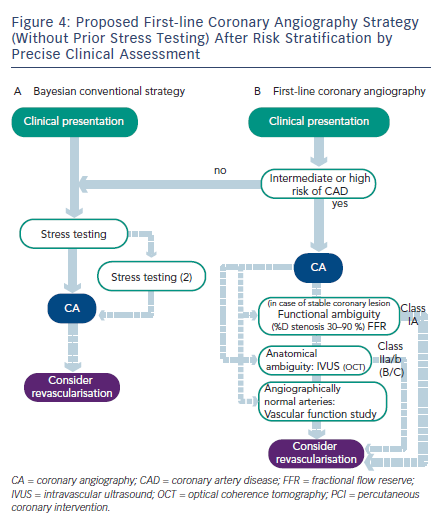 However, using FFR and its ability to analyse stenosis-by-stenosis and, more generally, artery-by-artery, several reports have demonstrated the locational imprecision of these tests in multivessel disease.45,46 These findings have a real impact on strategy, if myocardial revascularisation is indicated only on positive results on these non-invasive tests and on their topographic analysis, only partial revascularisation of myocardial ischaemia will be achieved (see Figure 2).
However, using FFR and its ability to analyse stenosis-by-stenosis and, more generally, artery-by-artery, several reports have demonstrated the locational imprecision of these tests in multivessel disease.45,46 These findings have a real impact on strategy, if myocardial revascularisation is indicated only on positive results on these non-invasive tests and on their topographic analysis, only partial revascularisation of myocardial ischaemia will be achieved (see Figure 2).
In acute coronary syndrome, the need for early treatment means that other lesions over and above the culprit lesion may be discovered, and frequently dilated without objective proof of ischaemia (see Figure 3).47
First-line Coronary Angiography – A Provocative Diagnostic Strategy?
There is a new strategy that should be mentioned and can now be argued for; implementing CA in first-line without preliminary noninvasive testing (see Figure 4). This attitude may seem at first glance to be provocative, but now in 2013 that is not really the case.
In reality, non-invasive tests are rarely performed ahead of angioplasty. The accuracy of non-invasive functional tests is often poor.48–51 The various stress imaging techniques (stress echocardiography, perfusion scintigraphy and cardiac magnetic resonance imaging [MRI] stress testing), while known to show better diagnostic performance than conventional exercise electrocardiography (ECG),52 seem to be less effective for locating myocardial ischaemia than artery-by-artery FFR measurement.45,46,53–55
Even so, CA performed without non-invasive testing in patients at intermediate or high-risk of clinically significant coronary disease will involve intrinsic anatomic and especially functional limitations. A decade ago, this attitude would have been difficult to defend; in the present day however, it is coherent – the twofold limitations of CA can and should be corrected by FFR and IVUS.56
First-line coronary angiography after risk stratification by precise clinical assessment can be an effective strategy,57 with:
Algorithms may be drawn up for a revascularisation strategy functionally determined by FFR and anatomically guided by IVUS.60