
Polymer-free Technology in Patients with Diabetes Mellitus – Procedure and Clinical Outcome
Rafael Romaguera of Barcelona, Spain, presented the case of a 62-yearold man with angina and DM, for which he was receiving insulin therapy. The patient was admitted with acute coronary syndrome (ACS) and 50–60 % stenosis in the LAD. The physician advised the patient that if a DES was used, he would do better than with BMS; that a secondgeneration DES is better than a first; that an EES has the most robust evidence of safety; and that he would be prescribed new antiplatelet drugs and statins. However, despite these interventions, he would remain at high risk of restenosis and adverse cardiovascular events. A 3.0 mm x 15 mm second-generation DES (zotarolim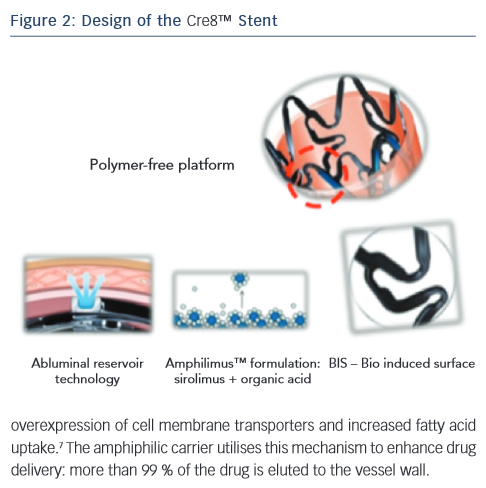 us-eluting stent [ZES]) was implanted. At 6-month follow up, the patient had stable angina. A 3.5 mm x 15 mm paclitaxel-eluting balloon was utilised to treat the restenotic lesion and the patient was discharged after experiencing no further events. However, 3 months later, the patient was readmitted due to an ACS and he was treated with crush stenting with a DES. The patient mentioned at the beginning of the presentation returned 3 months later with restenosis and received a stent of the left main. This patient was enrolled into the RESERVOIR clinical trial and received an AES.
us-eluting stent [ZES]) was implanted. At 6-month follow up, the patient had stable angina. A 3.5 mm x 15 mm paclitaxel-eluting balloon was utilised to treat the restenotic lesion and the patient was discharged after experiencing no further events. However, 3 months later, the patient was readmitted due to an ACS and he was treated with crush stenting with a DES. The patient mentioned at the beginning of the presentation returned 3 months later with restenosis and received a stent of the left main. This patient was enrolled into the RESERVOIR clinical trial and received an AES.
Dr Romaguera considered the causes of DES failure. Polymer-related inflammation is an important cause (see Figure 2). In addition, resistance to mammalian target of rapamycin (mTOR) inhibition is seen in patients with DM: a tenfold higher concentration of an mTOR inhibitor is needed in the diabetic cell to achieve similar inhibition to that seen in a non-diabetic one.6 The Cre8™ AES has unique features, making it well suited to patients with diabetes (see Figure 2). Among these, the amphiphilic carrier, which is a fatty acid, is a major component. Fatty acids play a main role in DM; cardiac cells cannot use glucose for energy generation as they are forced to utilise fatty acids. There is therefore an overexpression of cell membrane transporters and increased fatty acid uptake.7 The amphiphilic carrier utilises this mechanism to enhance drug delivery: more than 99 % of the drug is eluted to the vessel wall.
Dr Romaguera concluded by describing DM as the Achilles heel of interventional cardiology. Around 30 % of patients present with DM, and these patients need different DES characteristics, leading to the concept of a DES for patients with diabetes. The Cre8™ stent may fulfill this need as it has demonstrated unique efficacy in this population. However, it is important to remember that patients with DM will remain at high risk of adverse events due to disease progression in non-stented segments.
The publication of this article was supported by Alvimedica.