
Problem 1: Failed to deliver AXXESS
Delivery device failure should be considered a possibility when planning the case. However, with a careful strategy and appropriate equipment this risk is minimised. As detailed above, it is important to select a supportive guiding catheter along with good distal supportive guide-wires at the outset. Lesion preparation is crucial, with ideally 1:1 balloon sizing and predilation with NC, with or without cutting balloons as appropriate. Failure to prepare the vessel adequately is the most common reason for device delivery failure and can easily be overcome with more debulking. It is safe to remove the device if the cover sheath remains fully closed but caution should be taken once the distal stent is exposed. If this circumstance is encountered, it is safer to deploy in the main vessel rather than trying to remove the device once cover sheath retraction has commenced.
Problem 2: AXXESS Delivered too Proximally
Device being delivered too proximally can be a consequence of problem 1 or hasty device deployment. If this has occurred, with the struts clearly proximal to the carina and not spanning the ostium of either branch, then (after appropriate post dilatation as required) a second AXXESS device may be delivered through the first and placed in a more appropriate position distally. Care should be taken to remove the SB wire prior to AXXESS deployment to avoid wire trapping.
Problem 3: AXXESS Delivered too Distally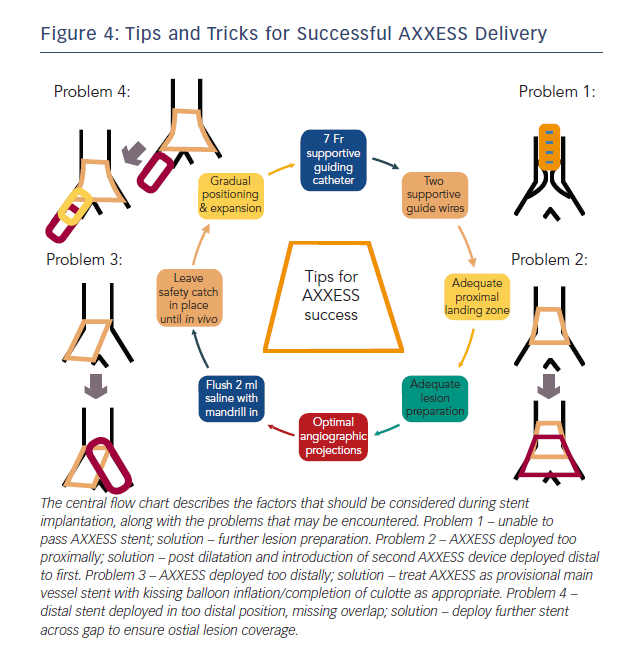
If the device is delivered too distally, it will be unable to expand fully and span across the carina. This may be corrected if the device is only just distal of the carina with a kissing balloon inflation that may flare the struts across the carina. If this is ineffective, or the device is positioned in such a way that this is clearly not possible, then it can be used safely and effectively as a provisional MV stent. The SB may be accessed through the device and the procedure completed using a culotte technique with FKBD if SB stenting is required or a provisional approach can be adopted.
Problem 4: Distal Stent Overlap
If a stent is required distally to the AXXESS device, then care should be taken with the positioning of the proximal stent edge to ensure overlap. If there is a suspicion that a gap remains between the two devices, then this should be confirmed using intracoronary imaging (intravascular ultrasound [IVUS] or optical coherence tomography [OCT]) and a further short stent used to cover as appropriate.
The majority of problems with the delivery and positioning of AXXESS can be predicted. By simply considering the factors detailed in Figure 4 when planning the procedure, the risk of a serious complication can be minimised.