
Coronary angiography has been the gold standard technique for evaluating coronary arterial disease for the past 50 years. Increasingly, however, realisation of the limitations of coronary angiography, mainly the inability to supply information regarding the coronary wall, has prompted the design and development of adjunctive technologies to better evaluate not just luminal disease but also the burden and character of atherosclerotic plaque within the vessel. The development of intracoronary imaging modalities, namely intravascular ultrasound (IVUS) and optical coherence tomography (OCT), has progressed quickly and these technologies now have established roles in the diagnosis and treatment of coronary artery disease. In general, intracoronary devices that can assess the coronary endothelium use either acoustic or optical signals that are received by a coronary catheter (IVUS uses ultrasound, OCT uses near-infrared light). This review addresses these two widely used intracoronary imaging techniques, looking at their clinical applications, recent evidence for their use and describes new developments in the field.
Intravascular Ultrasound
In the last 25 years IVUS has been established as the most commonly used intracoronary imaging device. An IVUS system cons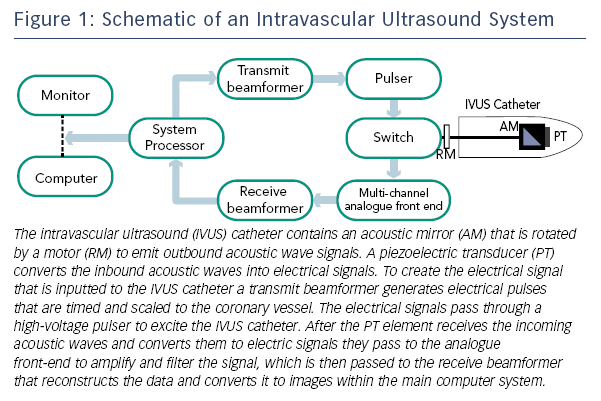 ists of a flexible monorail catheter with an ultrasound transducer at its tip that emits ultrasound waves in the 10–40 MHz range and an electronics console to reconstruct the image (see Figure 1).1 After reflection from tissue, part of the ultrasound energy returns to the transducer and is converted into the image.
ists of a flexible monorail catheter with an ultrasound transducer at its tip that emits ultrasound waves in the 10–40 MHz range and an electronics console to reconstruct the image (see Figure 1).1 After reflection from tissue, part of the ultrasound energy returns to the transducer and is converted into the image.
There are two types of IVUS transducers for clinical use: the mechanical rotating transducer and the electronically switched phased array system. The mechanical transducer uses a single crystal on a rotational device, which visualises the entire vessel in cross-section providing better image quality (compared with phased array technology) of 100–150 μm.2 The main disadvantage of mechanical transducers is the central drive shaft that decreases flexibility and prevents the concurrent use of a central guidewire.3 However, newer rotational IVUS catheters have developed a monorail system that allows for the presence of a central guidewire. Phased array catheters use multiple transducer elements, which are mounted along the circumference of the catheter tip. Each element sends and receives ultrasounds from a sector and multiple sectors are gathered to produce a cross-sectional image of the artery. However, they are disadvantaged by a technically complex set-up, requiring detailed programming;3 but some of the newer catheters are easier to set up.
Intracoronary imaging of coronary vessels by IVUS is performed using standard coronary interventional techniques and equipment (guiding catheter and 0.014 inch angioplasty guidewire) for catheter delivery along the guidewire beyond the target lesion/area of interest. Intravenous heparin and glyceryl trinitrate (nitroglycerin) are routinely administered before imaging. The IVUS catheter is then drawn back across the target lesion by either an automated pullback device (usually at a rate of 0.5–1.0 mm/s for any length) or by manual operator pull back. Importantly, as ultrasound waves pass through water and blood without major rebound signal, no coronary preparation is needed during image acquisition.
Safety of Intravascular Ultrasound
There is good evidence for the safety of IVUS use.4 Major complication rates (such as coronary artery dissection) are reported as <0.5 %.3 Minor complication rates vary from 1 to 3 % and are mainly due to coronary artery spasm, which is generally transient and responsive to intracoronary administration of nitrate.