
Comparison of the Two Techniques
IVUS provides useful information regarding vessel size, plaque morphology/area and can be used to guide the selection of interventional strategies; however, it is limited by image resolution. This is where OCT has demonstrated superiority with improved image resolution and contrast, and is therefore more attractive for the assessment of coronary arteries in further detail. The resolution of OCT (10–20 μm) is 10-fold higher than that of IVUS (100–150 μm); however, as a consequence, the penetration depth is lower (OCT: 1–2 mm compared with IVUS: 4–8 mm).25 Therefore, there is a limit in the ability of IVUS  to detect intimal tears, thrombus and stent malapposition (see Figure 5) whereas OCT has been demonstrated to visualise intimal hyperplasia, intraluminal thrombi, stent edge dissection and mural thrombus after PCI.22,45,46 Specific differences between OCT and IVUS are shown in Table 1.
to detect intimal tears, thrombus and stent malapposition (see Figure 5) whereas OCT has been demonstrated to visualise intimal hyperplasia, intraluminal thrombi, stent edge dissection and mural thrombus after PCI.22,45,46 Specific differences between OCT and IVUS are shown in Table 1.
With respect to plaque characterisation, OCT allows greater in-depth visualisation of detailed coronary struts including characteristics of coronary plaque (i.e. lipid-rich, fibrous and calcified plaques).25,26 However, in several applications, the shallower penetration of OCT may be a drawback. Whole vessel structures, including the external elastic lamina, cannot be visualised consistently by OCT, especially through lesions with a high amount of lipid-rich plaque burden. The relative merits of all the described intracoronary imaging modalities are shown in Table 2.
From a practical perspective one of the biggest differences between IVUS and OCT remains the need to replace the coronary blood pool with contrast during acquisition of OCT images. This involves the simultaneous injection of contrast to obtain the high definition images possible with OCT.47 The clinical value of the higher resolution images in guiding decision-making is still under evaluation.38
Studies Comparing Intrava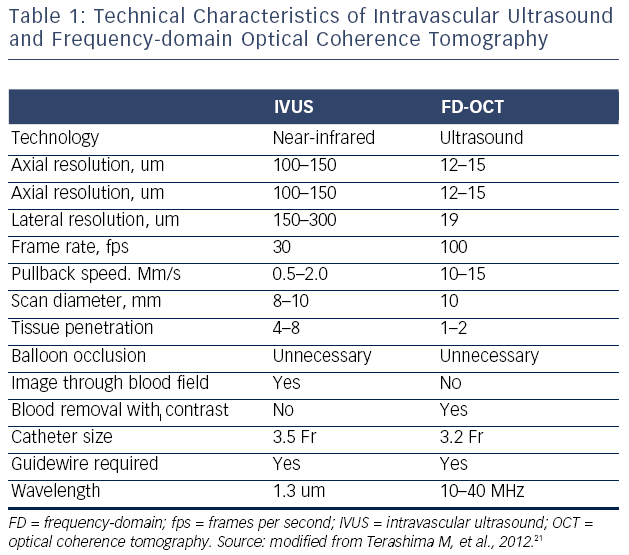 scular Ultrasound versus Optical Coherence Tomography
scular Ultrasound versus Optical Coherence Tomography
A recent prospective multicentre study (OCT Compared with IVUS in a Coronary Lesion Assessment [OPUS-CLASS] study) investigated the reliability of FD-OCT for coronary measurements compared with quantitative coronary angiography (QCA) and IVUS. Within a 100 patient cohort, both FD-OCT and IVUS exhibited good interobserver reproducibility, but the variability between measurements was approximately twice as high for the IVUS measurements as compared with the FD-OCT (0.32 versus 0.16 mm2).49 In addition, IVUS overestimated the lumen area and was less reproducible than FD-OCT (8.03 ± 0.58 mm2 versus 7.45 ± 0.17 mm2; p<0.001).49 FD-OCT therefore provided accurate and reproducible quantitative measurements of coronary dimensions in the clinical setting.
However, a recent randomised controlled trial comparing FD-OCT against IVUS for PCI optimisation reported that there was inferior stent expansion, both focal (65 versus 80 %, p=0.002) and diffuse (84 versus 99 %, p=0.003), when FD-OCT was used for guidance. PCI guided by FD-OCT also showed a significant increase in residual stent-edge plaque burden (51 versus 42 %, p<0.001). However, there were no significant differences in stent apposition.50 Therefore, this study found that IVUS had a significant advantage over OCT in terms of the reduction of residual stent-edge plaque burden and visibility of vessel border, which is in contrast to the results of the OPUS-CLASS study.49Table 3 is a summary of current clinical evidence for IVUS and OCT use.
Current Clinical Practice Guidelines 
The 2011 American College of Cardiology Foundation (ACCF)/American Heart Association (AHA)/Society for Cardiovascular Angiography and Interventions (SCAI) guidelines for PCI recommends the use of IVUS for the evaluation of angiographically indeterminate left main lesions and angiographically indeterminate (50–70 % stenosis) non-left main coronary lesions (Class IIa, Level of Evidence B recommendation).These guidelines also recommend the use of IVUS to evaluate the aetiology of stent restenosis and stent thrombosis (Class IIa, Level of Evidence C). The routine use of IVUS for evaluation of lesions when PCI is not planned was given a Class III recommendation.51
The 2010 European guidelines (European Society of Cardiology [ESC]) for Myocardial Revascularisation give a Class IIb, Level of Evidence C recommendation for the use of IVUS during unprotected left main PCI only.52 The lack of recommendation for other lesions or vessels appears to be related to limited data showing that IVUS reliably reduces MACE. However, the 2011 ACCF/AHA/SCAI guidelines do provide a Class IIa, Level of Evidence B recommendation for the use of IVUS for evaluation of donor coronary artery disease or allograft vasculopathy in post-cardiac transplantation patients.51
Currently neither the American (2011 ACCF/AHA/SCAI guidelines) nor European (ESC) guidelines provide recommendations for the routine use of OCT in clinical practice.51,52 However, more recent guidelines published in February 2014 by The National Institute for Health and Care Excellence (NICE)53 suggest that the evidence on the safety of OCT to guide PCI showed no major concerns. Due to the current available evidence on efficacy being limited in quantity and quality, it is recommended by NICE that this procedure should only be used with special arrangements for clinical governance, consent and audit or research.53
Future Clinical Research and Application of intra-coronary Imaging
OCT despite its extensive use in research studies has not yet been established in clinical practice and therefore currently should be seen as complementary to rather than replacing IVUS. However, it is expected that with the development of FD-OCT, the procedure will become both quicker and easier. As mentioned above, one major disadvantage of OCT is its limitation in the penetration depth (i.e. of approximately 2 mm). Therefore, although current OCT systems can demonstrate thin fibrous caps and thin neointimal coverage on DES, it is unable to quantify total plaque volume. Hence, development of new devices in conjunction with OCT might be helpful for both patient evaluation and clinical trials.
In addition, the need for optimal clearance of blood from the vessel lumen often requires extra doses of contrast to generate interpretable images. There are an increasing number of OCT studies being reported, which will hopefully further clarify the role of OCT in the near future. The FFR or OCT Guidance to RevasculariZe Intermediate Coronary Stenosis Using Angioplasty (FORZA) study will aim to compare the clinical and the economic impact of fractional flow reserve (FFR) versus OCT guidance in the percutaneous management of patients with angiographically intermediate coronary lesions.54 The DOCTORS study will evaluate the impact of changes in procedural strategy resulting from the use of OCT after angioplasty and stent implantation of a lesion responsible for NSTEACS.55
Finally, there has been little use of OCT in patients presenting with ST-elevation myocardial infarction (STEMI). Optical Coherence Tomography Assessment of Gender Diversity in Primary Angioplasty (OCTAVIA), is a recent study, which enrolled 140 STEMI patients who underwent primary PCI with an everolimus-eluting stent, and which demonstrated that at nine months, OCT showed that more than 90 % of patients had fully covered stent struts.56 Although this was a small study, it is likely that because of the superiority of OCT technology over IVUS, there will probably be many more studies that will use OCT to investigate plaque characterisation during primary PCI.
In addition to the rapid progress with OCT, future developments in IVUS are also expected with significant research ongoing indeveloping combinations of imaging modalities. Combining nearinfrared spectroscopy (NIRS) technology with IVUS allows better characterisation of lipid-rich plaque within a coronary artery.57 There are a number of ways by which NIRS-IVUS can help the optimisation of PCI and even play an important role in the prevention of spontaneous coronary events. Studies have suggested that NIRS has identified large, often circumferential lipid-rich plaques at the culprit site in most patients experiencing a STEMI.58 These data are now being translated into two large-scale prospective studies that will investigate the use of NIRS in the prediction of cardiac events beyond the success achieved with plaque burden in the PROSPECT Study.16,59