
Risk for Emergent Cardiac Surgery during TAVI
The most recent Valve Academic Research Consortium (VARC)-2 consensus document lists ECS among other TAVI-related complications, defined as any conversion to open sternotomy during the TAVI procedure secondary to any procedure-related complication. In the published literature, ECS is often defined as any cardiothoracic surgical intervention requiring cardiopulmonary bypass and sternotomy for urgent aortic valve replacement, repair of myocardial perforation or aortic injury, or pericardial drainage performed during or within 24 hours after TAVI.6 Nevertheless, definitions may be heterogenous throughout the literature.7 It may further be speculated that in some very-high-risk TAVI cases, ECS is not even attempted due to the anticipated bad outcome. Therefore, comparison of ECS rates between different studies may be hampered.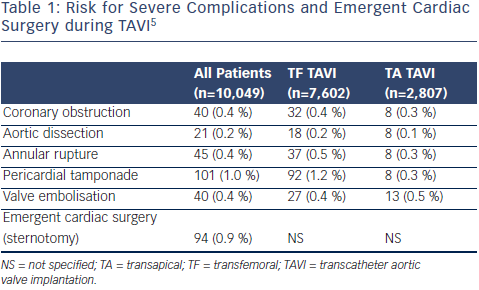
In a meta-analysis of 46 published studies comprising a total of 9,251 TAVI patients, ECS was required in 102 (1.1 %) patients.6 ECS rates were higher among patients undergoing TA TAVI compared with those undergoing TF TAVI.6,7 Contemporary national and international TAVI registries have yielded similar rates of ECS during TAVI. In the most recent report from the AQUA registry comprising 10,409 patients undergoing TAVI in Germany in 2013, ECS with sternotomy was required in 94 (0.9 %) patients.5 The FRANCE 2 registry reported that 12 out of 3,195 TAVI patients (0.4 %) were converted to open surgery.8 In a report from the initial US commercial experience, 94 (1.2 %) out of 7,710 patients underwent conversion to open heart surgery for TAVI complications.9 The international SOURCE registry using the balloonexpandable Edwards Sapien valve similarly reported an ECS rate of 1.2 %.10 More recently, the risk for ECS appeared even lower with a single (0.1 %) patient among a total of 995 patients included into the international ADVANCE registry.11 These patients were exclusively undergoing TF TAVI, using the self-expandable Medtronic/CoreValve prosthesis.11
Single-center experiences involving smaller numbers of patients have suggested higher ECS rates of up to 2.8 % or even 4.9 %.12,13 These numbers may in part be related to different definitions of ECS12 but also to the sites‚‘ TAVI experience/learning curve.14 Griese et al.12 reported that 20 (4.9 %) of 411 patients undergoing TAVI between 2009 and 2012 at their institution required ECS, including four patients who switched to TA TAVI (n=1) or femoral cardiopulmonary bypass for cardiogenic/hemorrhagic shock (n=3), but no sternotomy. There was also a strikingly high rate of ventricular perforation with either the pacing lead or the stiff guidewire with failed transcutaneous puncture ultimately necessitating ECS.12