
TAVI Complications Requiring Emergent Cardiac Surgery
Complications that occur during TAVI and require ECS include ventricular injury with tamponade (e.g. right or left ventricular perforation due to pacer lead or stiff guide wire), injury to the ascending aorta (e.g. perforation, dissection), rupture of the device landing zone (i.e. annular rupture), coronary obstruction, severe (para-)valvular regurgitation, and prosthesis embolization/migration into the left ventricle or aorta.7 The risk for these complications is generally low, ranging between 0.2 % and 1.0 % (see Table 1). In the German TAVI registry, which included 1,975 patients between 2009 and 2011, leading causes for ECS during TAVI were aortic injury (21 % of ECS cases), prosthesis embolization (21 %), and myocardial perforation (17 %).7 Similar distributions have been reported from the US TAVI registry, which included prosthesis embolization (23 % of ECS cases), aortic injury (13 %), and myocardial perforation (12 %), but also annular rupture (14 %) among the most frequent ECS causes.9 In the SOURCE registry of 2,307 patients, again prosthesis embolization (33 % of ECS cases) and aortic injury (26 %) were the main causes for ECS.10
Outcomes after Emergent Cardiac Surgery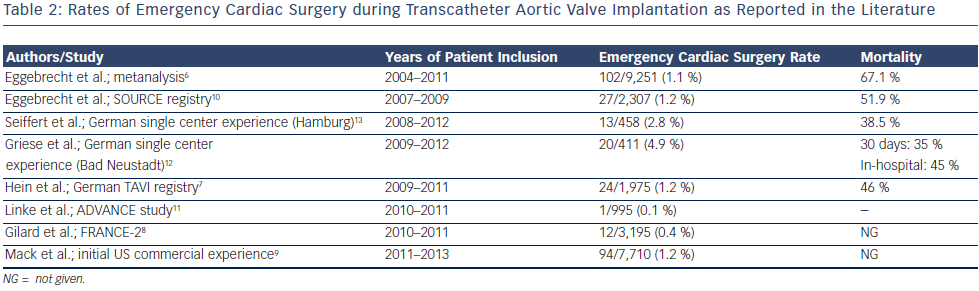
Patients currently selected for TAVI are usually elderly, co-morbid, and fragile patients deemed either inoperable or at least high risk for elective open heart surgery. It is therefore not surprising that mortality of emergency heart surgery for complications occurring acutely during the TAVI procedure is high. In fact, mortality among patients requiring ECS during TAVI may be as high as 67 %, thus being approximately ninefold higher than in patients undergoing uncomplicated TAVI.6 Other studies reported somewhat better outcomes after ECS, but the 30-day mortality rates still varied between 45 % and 52 %.7,10,12
It has been suggested that the severity of the specific TAVI complication that necessitates ECS has an effect on postoperative outcomes. In the German TAVI registry, the highest mortality was observed in patients undergoing ECS for aortic perforation or dissection: four (80 %) out of five patients died despite ECS.7 High mortality rates after ECS were also reported for annular rupture (50–100 %) and cardiac tamponade (50–100 %).7,10,15,16 By contrast, outcomes of patients with severe aortic regurgitation undergoing ECS appeared to be better: postoperative mortality ranged between 0 % and 33 %.7,10 As patients with severe aortic regurgitation are usually hemodynamically more stable than patients with overt annular rupture and tamponade, it may be speculated that not only the complexity of the complication, but also the hemodynamic status of the patient allowing for example more urgent/semi-elective instead of bail-out emergency surgery has an impact on postoperative outcomes. The analysis of Seiffert et al.13 further suggests that patients with a lower baseline risk (i.e. lower EuroSCORE) may have better outcomes even after ECS for TAVI complications.14