
A chronic total occlusion (CTO) in a coronary artery is defined as “the presence of TIMI 0 flow within an occluded arterial segment of greater than three months standing.”1 The successful percutaneous revascularisation of CTO vessels represents one of the dominant remaining technical challenges in interventional cardiology.
CTOs are common, found in between 20 %2 and 50 %3 of all patients with significant coronary artery disease (defined as a stenosis of >70 % in a single epicardial vessel). However, despite the frequency with which they are encountered, an attempt at revascularisation is made in only 10 % of cases.4 There remains a perception that CTO intervention is lengthy, costly, associated with significant risk and offers only limited clinical benefit. This is rooted in historical data demonstrating that both the procedural success and the long-term patency of CTO percutaneous coronary intervention (PCI) has been significantly lower when compared to non-CTO PCI.4 Almost certainly because of these data and reservations about CTO PCI, the culture h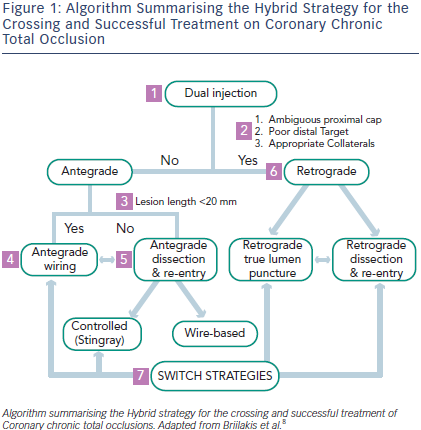 as developed that only a minority of CTO cases are considered for angioplasty. Most patients are therefore treated with simply medical therapy, thus condemning them to ongoing angina or coronary artery bypass surgery (CABG) surgery. Whilst surgery is an effective therapy for most patients, this is a longer procedure, with higher risk, longer recovery and there are recent concerns regarding long term graft patency specifically in the context of CTO.5
as developed that only a minority of CTO cases are considered for angioplasty. Most patients are therefore treated with simply medical therapy, thus condemning them to ongoing angina or coronary artery bypass surgery (CABG) surgery. Whilst surgery is an effective therapy for most patients, this is a longer procedure, with higher risk, longer recovery and there are recent concerns regarding long term graft patency specifically in the context of CTO.5
The traditional technical approach to CTO PCI is progressive antegrade wire escalation strategy. This remains technically challenging and has a high failure rate even in expert hands.4 Procedures are often lengthy and associated with high radiation doses for both patient and operator, as well as large volumes of radiographic contrast. Recent technical advances, including the adoption of dissection/re-entry6 and equipment to enable a retrograde approach7, have significantly increased procedural success rates. In addition, the new hybrid strategies (see Figure 1) have shortened procedure time, reduced contrast load, and decreased the need for repeat procedures7,8 (see Figure 1). Despite the perceived complexity of these techniques, they can be taught extremely effectively using an experienced proctor – and adopting such an approach can significantly improve success rates.9
Despite these advances, controversy persists regarding the objective clinical value of successful CTO PCI. The aim of this article is to critically examine the data that supports contemporary percutaneous CTO intervention, specifically including an evaluation of procedural safety and cost effectiveness.