
Prognostic Value of Troponin with Conventional Assays
The largest study examining cTn in AHF is the Acute Decompensated Heart Failure National Registry (ADHERE), an observational registry of heart failure hospitalisations at 274 hospitals.15 In an analysis of 67,924 patients, 4,240 (6.2 %) patients had a positive cTn test result on admission (cTnT >0.1 ug/l and cTnI >1 ug/l). Patients with a positive cTn test result had a lower systolic blood pressure on admission and a lower ejection fraction. These patients also had higher in-hospital mortality rates (8.0 %) versus those with a negative result (2.7 %), with an adjusted OR of 2.55 for risk of death (Figure 2). This increased risk persisted when adjusting for different in-hospital therapies, other known risk factors for increased mortality rates, and regardless of whether heart failure was ischaemic or non-ischaemic in origin. A limitation of this study was that the authors could not determine if the cTn level elevation was related to an ACS event. However, this is the largest study examining cTn in AHF showing definitively higher in-hospital mortality rates with an elevated cTn level.
Studies examining only cTnI in AHF have found increased risk of adverse events with an elevated level. In the EFFECT (Enhanced Feedback for Effective Cardiac Treatment)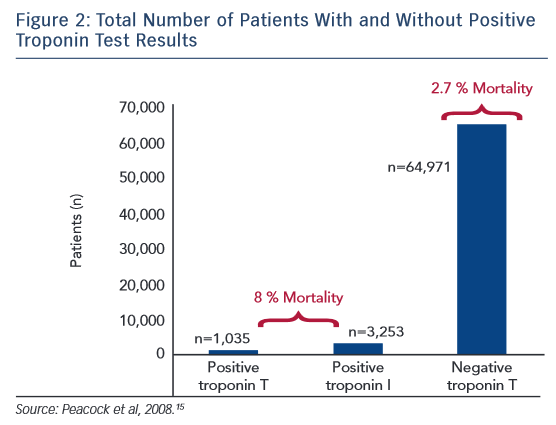 study involving 2,025 patients, a peak cTnI >0.5 ug/l measured in the first 48 hours of hospitalisation was an independent predictor of all-cause mortality at 1 year with an HR of 1.49.16 HR increased with cTnI level (1.1 per 1 ug/l increase) and this risk did not vary between patients presenting with or without acute ischaemia. Smaller studies have also demonstrated increased long-term mortality rates with an elevated cTnI level.17,18 An elevated cTnI level on admission has been associated with lower ejection fraction, higher systolic pulmonary artery pressure, and increased length of hospital stay.17,18 A persistently elevated cTnI level on repeated admissions, especially if >0.04 ng/ml, is associated with increased long-term mortality rates.19
study involving 2,025 patients, a peak cTnI >0.5 ug/l measured in the first 48 hours of hospitalisation was an independent predictor of all-cause mortality at 1 year with an HR of 1.49.16 HR increased with cTnI level (1.1 per 1 ug/l increase) and this risk did not vary between patients presenting with or without acute ischaemia. Smaller studies have also demonstrated increased long-term mortality rates with an elevated cTnI level.17,18 An elevated cTnI level on admission has been associated with lower ejection fraction, higher systolic pulmonary artery pressure, and increased length of hospital stay.17,18 A persistently elevated cTnI level on repeated admissions, especially if >0.04 ng/ml, is associated with increased long-term mortality rates.19
Similar to cTnI, elevated levels of cTnT in patients with AHF have demonstrated increased rates of adverse events. An elevated cTnT level (≥0.1 ng/ml) on admission has been associated with increased risks of heart failure readmission and mortality.20,21 These associations have been observed up to 3 years from the index hospitalisation when cTnT levels first became elevated.22 An elevated cTnT level at the time of discharge from a hospitalisation for AHF predicts an increased risk of heart failure exacerbation, cardiac death, and total mortality (HR of 5).23 Similar to cTnI, cTnT has prognostic use for mortality and morbidity risks.
Serial measurement of cTn levels during a hospitalisation for AHF has been repeatedly shown to have prognostic use. In the PROTECT (Placebo-controlled Randomized Study of the Selective A1 Adenosine Receptor Antagonist Rolofylline for Patients Hospitalized With Acute Decompensated Heart Failure and Volume Overload to Assess Treatment Effect on Congestion and Renal Function) study, serial cTnT were measured and patients were stratified based on baseline troponin level status (positive: >0.03 ng/ml; detectable: >0.01 ng/ml; negative: ≤0.01 ng/ml) as well as considered to have a conversion if cTn went from negative to detectable on serial sampling.24 On multi-variable analysis, patients with a positive cTn test result or conversion to a positive cTn had an increased risk of cardiovascular/renal rehospitalisation or death at 60 days compared with patients with a negative value. Similarly, in another study, an initially and persistently positive cTn value or a conversion to a positive cTn value was associated with increased risk of mortality, hospital readmission, and the combined endpoint of death and rehospitalisation.25 In the PRESERVD-HF (Pilot Randomized Study of Nesiritide Versus Dobutamine in Heart Failure) study, a significant proportion of patients were found to have an elevated cTn level on admission that rose during hospitalisation before falling or plateauing.26 The initial detectable and peak cTn levels were associated with worse short-term outcomes of death or worsening heart failure. These studies suggest serial measurements of cTn levels during hospitalisation may enhance its predictive value.
Other unique correlations have been found in patients with an elevated cTn level and presenting with AHF. An elevated cTnT level >0.2 ng/ml was associated with a longer left ventricular end-diastolic diameter and end-systolic diameter and a lower ejection fraction.27 An elevated systolic blood pressure and normal cTnI level (<2.0 ng/ml) was effective in identifying a population at low risk of experiencing adverse events that could be monitored in an observation unit.28 As detailed above, an elevated cTn level has been shown to predict mortality and readmissions and this predictive value has been retained as a significant variable in multiple models predicting death and readmission.29,30 Patients presenting with acute cardiogenic pulmonary oedema without MI who have a cTnT level >0.1 ng/ml are associated with a higher long-term mortality risk.31 Overall, the evidence overwhelmingly demonstrates that an elevated cTn level in patients with AHF predicts increased mortality as well as increased risk of readmission and correlation with more severe cardiac dysfunction.
Most studies examining elevated cTn with AHF have focused on patients with heart failure and reduced ejection fraction or combined patients with heart failure with reduced ejection fraction and preserved ejection fraction. Studies focusing solely on patients with AHF with preserved ejection and an elevated cTn level have also shown an association with worse outcomes compared with patients who have an undetectable cTn. In a subgroup analysis of patients with ejection fraction ≥45 % in the ALARM-HF (Acute Heart Failure Global Survey of Standard Treatment) study, an elevated cTnT level (>0.01 ng/ml) was predictive of increase in-hospital mortality rates.32 In another study involving a cohort of patients with an ejection fraction ≥40 %, a cTnT level ≥0.02 ng/ml was associated with worse clinical outcomes of death and rehospitalisation at 6 months with a HR of 1.8 compared with patients whose cTnT was <0.02.33 A study of patients with preserved ejection fraction showed an elevated cTn level to correlate with left ventricular end-diastolic dimension and tissue Doppler Ea wave peak velocity.34 Overall, these studies clearly show that an elevated cTn level in patients with AHF portends poor short- and longterm outcomes regardless of heart failure characteristics.