
Incidence of Sudden Cardiac Death in Athletes
The scale of the problem of SCD in athletes is difficult to define, as calculating the precise number of cases (numerator) and defining the exact reference population (denominator) is challenging in the absence of compulsory national or international registries. Studies have arrived at vastly different estimates varying from 1 per 300,000 per year5 to 1 per 23,000 per year.6 Differences in methodology and selection biases are largely responsible for this variation with available sources for case identification ranging from registries, sporting organisations, parent organisations, media reports or a combination of these. In addition, the estimate of 1 per 23,000 per year included both cases of SCD and survivors of sudden cardiac arrest (SCA),6 which is a more reasonable strategy as both SCD and SCA should be targeted by potential preventative strategies.
One large prospective study by Corrado et al. systematically assessed the incidence of SCD in young athletes.7 The study is unique as it prospectively studied a well-defined population of athletes and non-athletes in the Veneto region of Italy for 25 years. In contrast to all other studies, owing to the highly organised referral network, all deaths in young (aged 12–35 years) individuals considered to be of cardiac cause were referred for post-mortem evaluation to a single centre and underwent detailed cardiac histopathological evaluation by a small number of expert cardiac pathologists. Moreover, the unique pre-participation screening programme (PPS), which is enforced by law in Italy, ensures that athletes participating in formal competition are subjected to annual medical reviews. Based on the results of this study the incidence of SCD in young athletes was estimated at 1 per 24,000 per year prior to the initiation of the PPS,8 which is similar to that estimated by Drezner et al. in high school student athletes in the US.6
A consistent finding across all studies is that male athletes carry a higher risk of SCD than female athletes. The reasons for this are poorly understood. Although higher male participation rates in the most popular sports may partly account for this, gender-specific influences in disease expression are likely to contribute, as similar trends are observed in the general population.9 Black athletes also appear to suffer a disproportionately higher incidence of SCD. The National Collegiate Athletic Association in the US reported a three-fold higher risk in African-American athletes compared with Caucasian athletes (1 per 17,000 versus 1 per 58,000), with the highest incidence of SCD in male African-American athletes at 1 per 13,000 per year.10
By comparison, it is more difficult to investigate SCD rates in recreational and veteran athletes, as the reporting of these deaths is less consistent and in many cases unlikely to be witnessed. As a result, there are relatively fewer studies evaluating the incidence of SCD in older athletes. A comprehensive, prospective 5-year study of sports-related SCD in the French general population revealed that the overwhelming majority of sports-related SCD occurred among those aged ≥35 years and was greatest in the fifth decade of life. In this study, the overall burden of sports-related SCD was 4 .6 deaths per million population per year, with only 6 % occurring in young competitive athletes.11 In a more recent study by the same group the incidence of sports-related SCA increased to 21.7 per million population per year when focusing on middle-aged individuals (aged 35–65 years).12
.6 deaths per million population per year, with only 6 % occurring in young competitive athletes.11 In a more recent study by the same group the incidence of sports-related SCA increased to 21.7 per million population per year when focusing on middle-aged individuals (aged 35–65 years).12
Aetiology of SCD in Athletes
Causes of Sudden Cardiac Death in Young Athletes
The causes of SCD in athletes are divided based on the age of the athlete; the age of 35 years is used as the cut-off point. In athletes ≤35 years of age, inherited or potentially inherited cardiac diseases account for most SCDs. There is, however, disparity across different registries as to the most common cause of SCD.1 In the US registry from the Minneapolis Heart Institute Foundation, hypertrophic cardiomyopathy (HCM) was the most common cause of death, accounting for 36 % of SCDs in this population. Coronary artery anomalies of abnormal origin were next in frequency at 17 % and arrhythmogenic right ventricular cardiomyopathy (ARVC) was responsible for only 4 % of deaths. Other causes of SCD such as myocarditis, ion channelopathies, coronary artery disease (CAD), dilated cardiomyopathy, mitral valve prolapse, aortic stenosis and aortic rupture each accounted for ≤6 % of SCDs (see Figure 1).14
In comparison, the results of the registry in the Veneto region of Italy place ARVC as the most common cause of SCD (23 %), followed by atherosclerotic CAD (19 %).7 Anomalous origin of the coronary arteries accounted for 13 % of SCDs, with mitral valve prolapse contributing 12 %, myocarditis 10 % and conduction system disease 8 % (see Figure 1).7 Although the Italian registry is smaller in scale compared with the US registry, the accuracy of diagnoses by specialist cardiac pathologists give additional credibility to the results. Variations between the findings in each registry may be explained in part by the differences in the population, differences in methodology relating to data collection and interpretation of autopsy findings and the fact that systematic PPS of athletes in Italy may have prevented SCDs due to HCM through the disqualification of affected athletes.
Contemporary Studies of Causes of SuddenCardiac Death in Athletes
Contemporary studies have further added to the diversity of SCD causes in athletes and highlighted the complexity of the subject. Post-mortem examination of 89 young athletes in 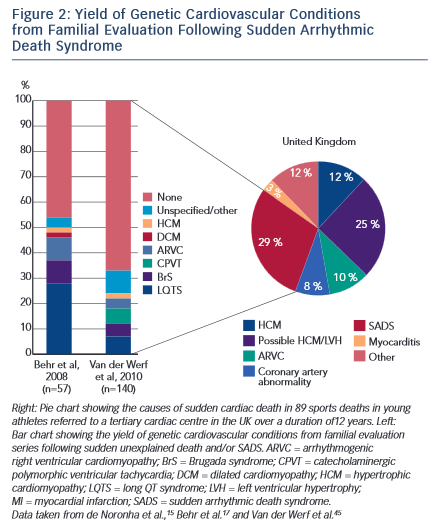 the UK suffering SCD revealed a normal heart as the most common finding, implicated in almost a third (29 %) of deaths.15 Other novel entities included idiopathic left ventricular hypertrophy (LVH) and idiopathic fibrosis accounting for 25 % and 7 % of SCDs, respectively. Established cardiomyopathies such as HCM and ARVC accounted for 22 % of cases, while coronary artery pathology was present in 8 % of deaths (see Figure 2).15 Although the high prevalence of autopsy-negative SCDs in the UK study may be in part attributed to significant referral bias, further studies have reported similar results. Of the 45 SCDs in US college athletes, a structurally normal heart was the most common finding at post-mortem accounting for 31 % of cases, while idiopathic LVH was present in 8 %.13 Similarly, a 25-year review of deaths in young military recruits in the US, identified autopsy-negative sudden unexplained death in 30 % of cases (see Figure 1).16
the UK suffering SCD revealed a normal heart as the most common finding, implicated in almost a third (29 %) of deaths.15 Other novel entities included idiopathic left ventricular hypertrophy (LVH) and idiopathic fibrosis accounting for 25 % and 7 % of SCDs, respectively. Established cardiomyopathies such as HCM and ARVC accounted for 22 % of cases, while coronary artery pathology was present in 8 % of deaths (see Figure 2).15 Although the high prevalence of autopsy-negative SCDs in the UK study may be in part attributed to significant referral bias, further studies have reported similar results. Of the 45 SCDs in US college athletes, a structurally normal heart was the most common finding at post-mortem accounting for 31 % of cases, while idiopathic LVH was present in 8 %.13 Similarly, a 25-year review of deaths in young military recruits in the US, identified autopsy-negative sudden unexplained death in 30 % of cases (see Figure 1).16
Recognition of a normal heart on autopsy, also referred as sudden arrhythmic death syndrome (SADS), is of paramount importance given its association with inherited ion channelopathies.17 Studies on familial evaluation after a SADS death have demonstrated evidence of an ion channelopathy or cardiomyopathy in up to 50 % of families (see Figure 2).17 In addition, the significance of idiopathic LVH and idiopathic fibrosis remains uncertain and postulated theories include being innocent bystanders, pathological variants of physiological LVH in genetically predisposed individuals or part of the HCM spectrum.18 In athletes with normal hearts or autopsy findings of uncertain significance the contribution of severe metabolic or electrolyte disturbances and heatstroke must also be taken into consideration as potential causes of sudden death. One study examining life-threatening and fatal events occurring during endurance races in Israel over a 6-year period found that heatstroke was responsible for the majority of events.19
Causes of Sudden Cardiac Death in Older Athletes
The predominant cause of SCD in athletes aged >35 years is atherosclerotic coronary artery disease (CAD), identified in more than 80 % of cases.20 Acute exercise can lead to transient activation of the coagulation system, which promotes a pro-thrombotic environment.21 Additional metabolic and haemodynamic changes during exercise may contribute to stress-related plaque rupture observed in sports- related victims of SCD.22 On post-mortem examination, coronary atheroma with significant luminal obstruction (>75 %) may be present,23,24 with associated features indicative of acute or chronic myocardial infarction. However, plaque rupture, thrombosis, acute infarction and fibrosis are not prerequisites for the cause of death to be attributable to CAD. In such cases, the presumed mode of SCD is sudden ventricular arrhythmia due to myocardial perfusion-demand mismatch and resultant ischaemia.25