
Pre-participation Cardiac Evaluation of Older Athletes
The rapidly expanding population of older veteran or amateur athletes who compete in high-intensity events underscores the importance of preventing SCD in this age group. The resting 12-lead ECG is of limited value in screening senior athletes, as CAD is the main cause of SCD.36 The Sports Cardiology section of the European Association of Cardiovascular Prevention and Rehabilitation published recommendations relating to screening practices, which take into account the burden of cardiovascular risk factors, pre-existing fitness levels and intended level of exercise.37 The assessment of athletes undertaking high intensity physical activity incorporates the assessment of cardiovascular risk factors, symptoms and family history; physical examination; resting 12-lead ECG; and the Systematic Coronary Risk Evaluation (SCORE) to assess the 10-year risk of a fatal cardiovascular event. Any abnormalities arising from this initial assessment, including a SCORE 10-year risk of ≥5 %, requires maximal exercise ECG testing. However, it is well recognised that the sensitivity of exercise ECG stress testing in a screening setting with predominantly asymptomatic individuals is poor (25 %)38 and the false-positive rates are high, particularly in women.39 Nevertheless, a negative maximal exercise ECG stress test provides eligibility for moderate/high exercise training and a positive test result will require further investigation for underlying CAD, the gold standard test being invasive coronary angiography (see Figure 3B).
An area deserving further consideration is whether computed tomography coronary artery calcium scoring (CACS) can provide a better risk prediction of serious cardiovascular events, as high calcium scores appear to predict increased risk for cardiovascular events in the general population,24 including asymptomatic individuals.40 Obstacles to the wider implementation of CACS as a screening tool include radiation exposure (though minimal at 1.5–3.0 mSv), availability and cost.
Evaluation of the Patient and the Family
The inherited nature of most conditions predisposing to SCD in young athletes highlights the importance of comprehensive post-mortem evaluation of the index case as well as cardiovascular screening of first-degree relatives.
The importance of a histopathological examination by a cardiac pathologist with expertise in the morphological adaptations of the athletic heart and disease phenotypes implicated in SCD in athletes cannot be overstated, as false conclusions may misguide fam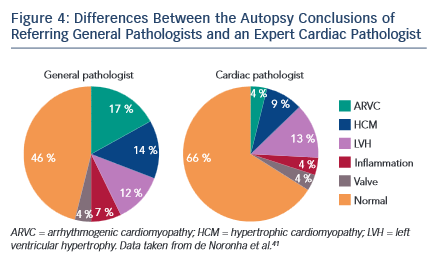 ilial evaluation or offer false reassurance to surviving relatives and dissuade physicians from initiating familial screening. When comparing the cause of death attributed to a series of SCDs, there was a disparity in 41 % of cases between the referring pathologists and the specialist pathologist41. Referring pathologists were more inclined to diagnose cardiomyopathy than morphologically normal heart, with only 63 % of normal hearts being described correctly (see Figure 4). Examples of misdiagnoses can include post-mortem coronary artery collapse with mild atheroma being mislabelled as CAD; overdiagnosis of ARVC where right ventricular fatty infiltration is related to obesity, alcohol misuse or other causes; and overdiagnosis of HCM in hypertrophied hearts despite the absence of myocyte diasarray.18 A guideline has been developed by the Association for European Cardiovascular Pathology to reduce variation in practice and to provide a minimum standard, ensuring accurate, systematic examination and sampling in the autopsy investigation of SCD.42
ilial evaluation or offer false reassurance to surviving relatives and dissuade physicians from initiating familial screening. When comparing the cause of death attributed to a series of SCDs, there was a disparity in 41 % of cases between the referring pathologists and the specialist pathologist41. Referring pathologists were more inclined to diagnose cardiomyopathy than morphologically normal heart, with only 63 % of normal hearts being described correctly (see Figure 4). Examples of misdiagnoses can include post-mortem coronary artery collapse with mild atheroma being mislabelled as CAD; overdiagnosis of ARVC where right ventricular fatty infiltration is related to obesity, alcohol misuse or other causes; and overdiagnosis of HCM in hypertrophied hearts despite the absence of myocyte diasarray.18 A guideline has been developed by the Association for European Cardiovascular Pathology to reduce variation in practice and to provide a minimum standard, ensuring accurate, systematic examination and sampling in the autopsy investigation of SCD.42
The retention at post mortem of blood or splenic tissue allows for genetic testing, which is referred to as molecular autopsy. Genetic mutations can be identified and may be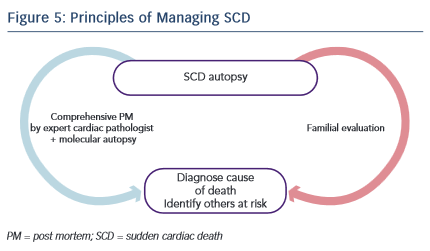 highly relevant and potentially informative as to the possible cause of SCD, and can facilitate clinical and genetic screening of family members to identify those at risk. Molecular autopsy opens the possibility to investigate ion-channel disorders such as long-QT syndrome, catecholaminergic polymorphic ventricular tachycardia and Brugada syndrome at post mortem, where the heart is unlikely to demonstrate any structural abnormality, also referred to as SADS.
highly relevant and potentially informative as to the possible cause of SCD, and can facilitate clinical and genetic screening of family members to identify those at risk. Molecular autopsy opens the possibility to investigate ion-channel disorders such as long-QT syndrome, catecholaminergic polymorphic ventricular tachycardia and Brugada syndrome at post mortem, where the heart is unlikely to demonstrate any structural abnormality, also referred to as SADS.
Complementary to the process of establishing an accurate cause of death is the process of investigating first-degree family members (see Figure 5). Where a clear cause of death is established by histopathological examination or molecular autopsy, targeted investigations suited to the detection of that condition can be applied to the relatives of the SCD patient. In cases where no clear cause has been found at autopsy, or the autopsy revealed a morphologically normal heart, investigations are used sequentially to assess for the presence of cardiomyopathy or an inheritable arrhythmogenic condition. First-line assessment includes history, physical examination, resting 12-lead ECG, transthoracic echocardiography, exercise tolerance testing and 24h-Holter ECG monitoring. The use of further tests is predicated upon the findings of the first-line assessment. Up to 25 % of relatives of patients with SADS are diagnosed with a previously unsuspected inherited cardiac condition17 and interventions ranging from simple lifestyle modification advice to the implantation of a prophylactic implantable cardioverter- defibrillator can reduce the risk of further fatalities.
Secondary Prevention Strategies
Emergency Response Planning
A comprehensive medical action plan that is rehearsed on a regular basis is essential to ensure the best possible outcome in the context of SCA in sports arenas.43 The importance of an effective emergency response plan is underscored by studies that have demonstrated that prompt CPR and defibrillation of athletes (within 5 minutes) resulted in survival rates in excess of 60 %.6 The same message is reiterated by studies of sports-related SCA in the general population, where a witnessed event, prompt CPR and the use of a cardiac defibrillator ventricular fibrillation were associated with higher survival to hospital discharge.11,12
The Fédération Internationale de Football Association (FIFA) support and promote a standardised and consistent level of advanced life support and emergency medical care on the football field, including a FIFA universal medical emergency bag and an ‘11-step plan to prevent SCD’. The ‘FIFA 11 steps’ include primary prevention with PPS, training of personnel on CPR, availability of AEDs, rehearsal of the emergency medical plan on an annual basis, equipment checks, logistical planning and protocols designed to enhance the resuscitation team’s performance.44