
Diabetes Mellitus and Heart Failure Diagnosis
As HF diagnosis is based on the combination of clinical data and diagnostic tests, BNP levels can help to distinguish between 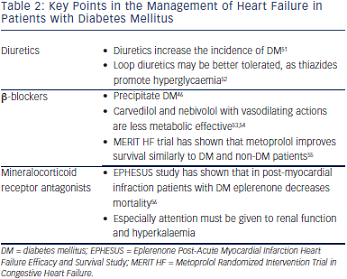 cardiac and non-cardiac causes of acute dyspnoea in the emergency department.47 BNP levels and reference limits can be affected by several factors such as age, obesity, renal impairment, etc.48 Nevertheless, data from the Breathing Not Properly Multinational Trial suggest that diabetes status is not a confounding variable to be considered when interpreting BNP concentrations in patients who present acutely with dyspnoea.47 However, in asymptomatic diabetic patients there was no significant difference among non-HF patients, HF patients and those with a HF history,49 and no conclusions could be rendered as to the role of BNP testing for screening asymptomatic diabetic patients for left ventricular dysfunction because the degree of disease severity among the diabetic patients could not be assessed. Therefore, in the diagnostic work-up of diabetic patients presented not emergently in primary care centres, we must follow the diagnostic algorithm proposed by the guidelines, which emphasises that patients with high pre-test likelihood of HF may be referred directly for echocardiography.5
cardiac and non-cardiac causes of acute dyspnoea in the emergency department.47 BNP levels and reference limits can be affected by several factors such as age, obesity, renal impairment, etc.48 Nevertheless, data from the Breathing Not Properly Multinational Trial suggest that diabetes status is not a confounding variable to be considered when interpreting BNP concentrations in patients who present acutely with dyspnoea.47 However, in asymptomatic diabetic patients there was no significant difference among non-HF patients, HF patients and those with a HF history,49 and no conclusions could be rendered as to the role of BNP testing for screening asymptomatic diabetic patients for left ventricular dysfunction because the degree of disease severity among the diabetic patients could not be assessed. Therefore, in the diagnostic work-up of diabetic patients presented not emergently in primary care centres, we must follow the diagnostic algorithm proposed by the guidelines, which emphasises that patients with high pre-test likelihood of HF may be referred directly for echocardiography.5
Moreover, clinicians should not overlook that DM patients with stable coronary heart disease may present with atypical symptoms, such as shortness of breath. Accordingly, we must be cautious in the interpretation of dyspnoea in these patients.50
Management of Heart Failure and Diabetes Mellitus
As both entities (HF and DM) are characterised by high morbidity and mortality, efforts for the best possible management must be taken. Nevertheless, treatment of HF may adversely interact with DM and vice versa (see Tables 2 and 3).
Heart Failure Treatment – Interaction with Diabetes Mellitus

Diuretics
Diuretics, especially furosemide, are one of the most useful treatments in HF patients for symptom relief and are used to achieve euvolaemia.5 Data from studies and meta-analyses (mostly in hypertensive subjects) suggest an association between incident diabetes and diuretics.46 Hypokalaemia, changes in autonomic nervous system function, in beta (β)-cell insulin release and in insulin’s peripheral effects are the proposed mechanisms.51,68 Accordingly, in HF patients under diuretic treatment attention to keep potassium levels and glycaemic status under control must be attained. Thiazides have been shown to promote hyperglycaemia and loop diuretics may be better tolerated in DM patients.52
Beta-blockers
Beta (β)-blockers especially when they are combined with diuretics can precipitate DM.46 Newer β-blockers with vasodilating actions, such as carvedilol and nebivolol, are less metabolic effective compared with metoprolol, do not affect glycaemic control and improve some components of the metabolic syndrome through improvement of the oxidative stress, insulin sensitivity and adiponectin levels.53,54. Vasodilating b-blockers increase survival in HF patients5 and should be preferred in patients with DM. Another β-blocker that can improve survival and symptoms in HF is metoprolol. Although it adversely affects insulin sensitivity, the Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF) trial has shown that it can reduce mortality and HF symptoms similar to DM and non-DM patients.55 A recent prospective study in HF patients with DM also concluded that metoprolol is highly safe and tolerable, and can remarkably improve the clinical status of the patients.69
Mineralocorticoid Receptor Antagonists
Eplerenone is a novel minelarocorticoid receptor antagonist, which is useful in HF patients. Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) in patients after acute myocardial infarction, ejection fraction <40 % and DM revealed that eplerenone on top of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers can decrease mortality.56 As renal dysfunction frequently co-exists with DM and HF,70 attention to renal function and hyperkalaemia must be applied when the combination of eplerenone and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers are used.