
Treatment of Symptomatic Left Ventricular Outflow Tract Obstruction
Currently, there is no evidence that asymptomatic patients with LVOTO benefit from treatment to reduce the seve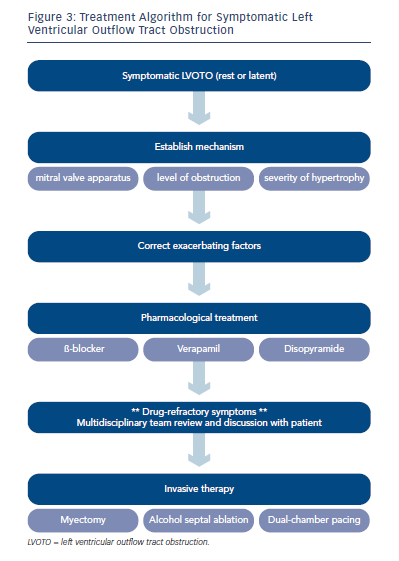 rity of obstruction; treatment is reserved for patients with LVOTO and drug-refractory symptoms.43,44 A contemporary treatment algorithm for symptomatic patients with LVOTO is summarised in Figure 3. The first-line treatment for symptoms associated with LVOTO is correction of exacerbating factors (e.g. vasodilating antihypertensives, anaemia) followed by pharmacological therapy with β-blockers, verapamil and disopyramide, which modulate the dynamic physiology of obstruction through their negative inotropic and chronotropic effects.43–46 In patients with drug-refractory symptoms or unacceptable side effects, invasive treatments should be considered by a multidisciplinary team following a comprehensive evaluation of the mechanism of obstruction:
rity of obstruction; treatment is reserved for patients with LVOTO and drug-refractory symptoms.43,44 A contemporary treatment algorithm for symptomatic patients with LVOTO is summarised in Figure 3. The first-line treatment for symptoms associated with LVOTO is correction of exacerbating factors (e.g. vasodilating antihypertensives, anaemia) followed by pharmacological therapy with β-blockers, verapamil and disopyramide, which modulate the dynamic physiology of obstruction through their negative inotropic and chronotropic effects.43–46 In patients with drug-refractory symptoms or unacceptable side effects, invasive treatments should be considered by a multidisciplinary team following a comprehensive evaluation of the mechanism of obstruction:
ASA is currently the most frequently used invasive therapy, and while it is efficacious, relatively safe and minimally invasive, outcomes from randomised trials comparing different invasive techniques are not yet available. Several experienced opinions still regard surgical treatment as the ‘gold standard’.43,44 Currently, patients must be counselled that choices between ASA, surgery and pacing are made on the basis of considerations other than proven differences in outcome.
In general, ASA may be unsuitable in the presence of co-existing mid-cavity obstruction and/or intrinsic mitral valve disease; in such cases a surgical approach should be considered. Septal reduction either by ASA or myectomy when the septal wall thickness is <15 mm at the site of mitral contact is also challenging, and alternatives such as mitral valve repair/replacement or AV sequential pacing should be considered. AV sequential pacing can also be useful in selected patients where aggressive pharmacological treatment with a β-blocker, verapamil and disopyramide is contemplated, and in patients too frail to tolerate more invasive treatment. In others, pacing may be considered as an initial therapeutic trial before progression to more invasive treatment. This may include individuals with conventional indicators for device therapy (including pacing and defibrillator treatment) and patients at high risk of developing heart block following invasive treatment. Patient preference is also a key factor in decision-making.