
Alcohol Septal Ablation – Procedural Aspects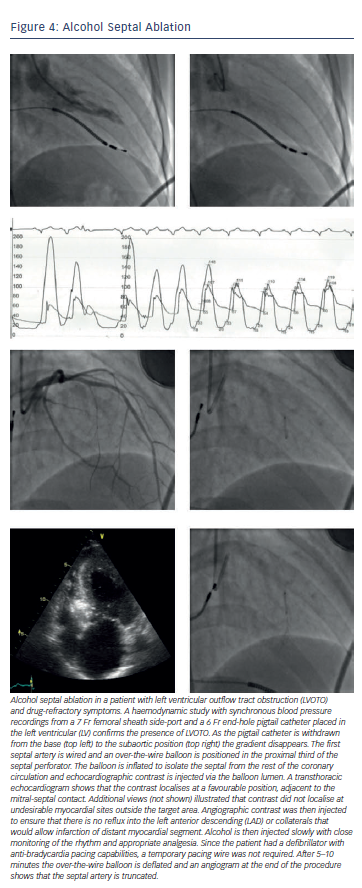
The essential components of this percutaneous procedure include the identification of an appropriate septal perforator artery, its isolation from the rest of the coronary circulation and the selective injection of alcohol into this artery. The first septal artery is usually selected and a short over-the-wire balloon inflated within the artery. The balloon’s lumen allows selective delivery of angiographic contrast, echo contrast and ultimately, alcohol into the septal artery. Angiographic contrast ensures that the septal artery is isolated from the left anterior descending (LAD) by the inflated balloon, and echo contrast confirms that the myocardial volume subtended by the selected septal artery is an appropriate target for ablation.63–65 The proximal septal vessels may also supply the right ventricular free wall, LV apex and papillary muscles, and several echocardiographic views are needed to ensure contrast enhancement is confined to the target area; the appropriate target lies adjacent to the point of mitral-septal contact. If echo contrast does not localise to the target area, other septal arteries should be selectively assessed. A temporary pacing wire is inserted prior to the injection of alcohol in case significant bradyarrhythmias follow conduction system damage. Right bundle branch block is observed in approximately 50 % of cases.66 Adequate analgesia is provided and the alcohol is slowly injected to chemically ablate and infarct the target myocardium.67 Approximately 0.1 ml of ethanol (concentration >95 %) per 1 mm of thickness of the target myocardium is injected slowly (1 ml/minute).64 The balloon remains inflated for 5–10 minutes postethanol injection to prevent reflux in the anterior descending and to enhance delivery at the target myocardium. LVOTO is often reduced or abolished at the end of the procedure; this acute effect reflects septal stunning, and the LVOT gradient may again increase in the days following the procedure, to fall again over a period of weeks as septal remodelling occurs and a small scar develops in place of the ablated myocardium. The femoral or radial approach can be used.68 Important procedural steps are shown in Figure 4.
Acute Complications of Alcohol Septal Ablation
Since its inception in 1995,55 ASA has evolved and the routine use of echo contrast to select the target septal artery has made the procedure safer and more effective.63–65 In addition to complications arising from the injection of alcohol, ASA is also associated with the complications of percutaneous coronary intervention and temporary wire insertion:
Despite these potential complications, ASA remains a relatively safe procedure with in-hospital death rates of around 1 %.69,75