
Introduction on Takotsubo Cardiomyopathy
Takotsubo cardiomyopathy (TTC) has gained more recognition since its first description in 1990 by Satoh et al.1,2 The word takotsubo refers to the Japanese octopus trapping pot with a large round base and narrow neck, which is the characteristic shape of the left ventricle (LV) in this syndrome, although other morphologies have since been described.3 TTC is known by many names including stress cardiomyopathy, broken heart syndrome, apical ballooning syndrome and ampulla cardiomyopathy. It is a reversible form of cardiomyopathy that presents clinically as an acute myocardial infarction (MI) triggered by an emotionally or physically stressful event. An abnormal 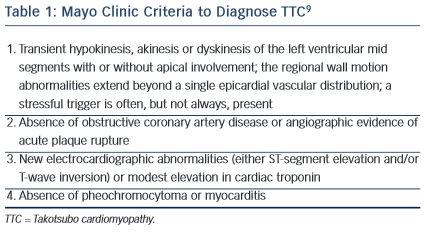 response to a catecholamine surge leads to TTC and a stressor can be identified in a majority of cases. TTC occurs at a significantly higher frequency in post-menopausal women with 80–85 % of all cases presenting in women. Less than 3 % of cases occur in those less than 50 years of age.4
response to a catecholamine surge leads to TTC and a stressor can be identified in a majority of cases. TTC occurs at a significantly higher frequency in post-menopausal women with 80–85 % of all cases presenting in women. Less than 3 % of cases occur in those less than 50 years of age.4
The exact incidence of TTC is unknown since it is likely under-diagnosed. The annual rate is between 7,000–14,000 cases per year in the US and it is estimated that 1–2 % of acute coronary syndrome (ACS) diagnosed in the US is actually TTC.4,5 The Nationwide Inpatient Sample (NIS) database in 2008 found that 0.02 % of all hospitalisations in the US were attributed to TTC.5 This study also found that hyperlipidaemia, active smoking, alcohol abuse, anxiety and stress were associated with TTC.5 One study found significantly lower cardiovascular risk factors in TTC patients compared with population-matched MI patients.6 On the contrary, the recently published systematic review of TTC patients, known as the COmorbidity freqUency iN Takotsubo Syndrome (COUNTS) study, reported a high prevalence of cardiovascular risk factors in TTC patients compared with the general population.7,8 Out of the 1,109 patients in this study, on average 17 % were obese, 54 % had hypertension, 32 % hyperlipidaemia, 17 % were people with diabetes and 22 % were smokers.7 Common comorbidities reported in TTC patients include malignancy, neurological disorders including stroke, pulmonary diseases, chronic kidney disease, thyroid disease and psychological disorders.7 Unlike the study by El-Sayed et al., the COUNTS study reports a poor association between TTC and drug abuse, chronic liver disease and sepsis.6,7 Interestingly, TTC cases occurred at a higher rate in July in contrast to acute MIs, which peak in occurrence in winter months.5 The exact reasons for this potential seasonal variation in TTC are unknown.
The Mayo Clinic proposed criteria in 2004 for diagnosing TTC (see Table 1).9 They suggested that all four criteria should be present in order to diagnose TTC. In 2006 the American Heart Association (AHA) classified TTC as a primary acquired cardiomyopathy.